
17 Questions to Ask About Your Epidural (Before You’re in Labor)
More than 75% of women in the United States receive an epidural during labor. Most of them were never given the evidence. Here is what the data actually shows.

She had done everything right.
She had written a birth plan. She had taken the hospital’s childbirth class. She had read three books, watched hours of YouTube videos, and hired a doula. She had decided, firmly, that she did not want an epidural.
Then labor started. At 5 centimeters, the contractions were coming every two minutes. She asked for the epidural. The anesthesiologist arrived 47 minutes later. Within 20 minutes, her pain dropped from a 9 to a 2. She delivered vaginally four hours later without complications.
Afterward, she cried. Not from joy. From guilt.
Her mother-in-law told her the epidural had “slowed everything down.” A friend texted that epidurals “make cesareans more likely.” An Instagram post she had saved months ago said epidurals “interfere with bonding.” None of these claims were supported by the evidence she had never been shown.
She had made a perfectly reasonable medical decision. And the people around her, armed with myths instead of data, made her feel like she had failed.
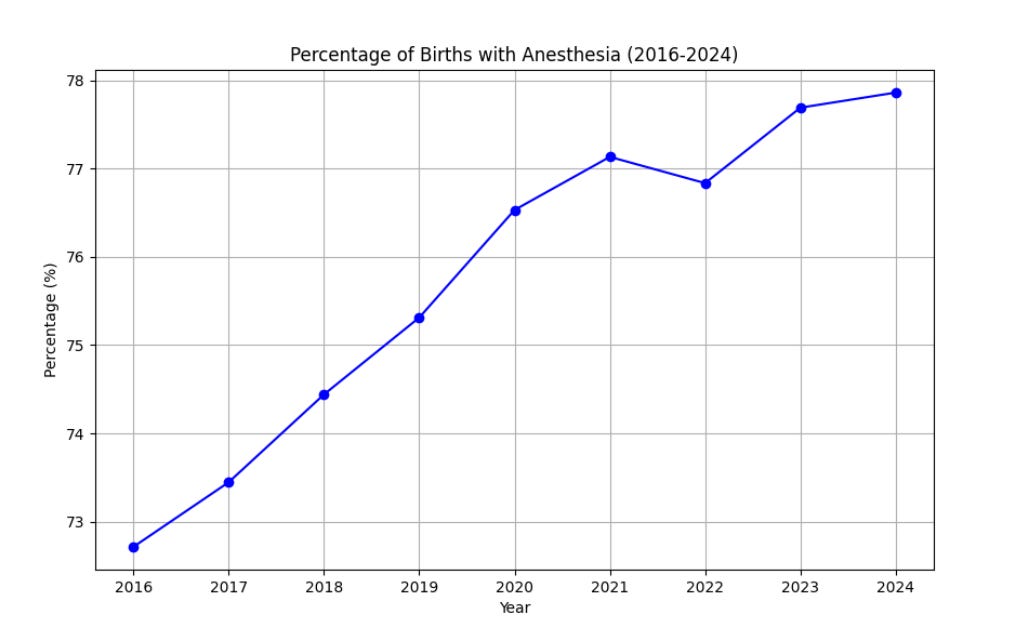
This graph shows data from the CDC birth database showing nearly 80% (4 in 5 or 80 in 100) had an epidural as of 2024, up from 72% in 2016.
The Gap Between Fear and Evidence
Epidural analgesia is the single most effective form of pain relief available during labor. The 2018 Cochrane review, which pooled data from 40 randomized controlled trials involving more than 11,000 women, found that epidurals reduce pain scores dramatically compared to opioid analgesia or no analgesia (1). Women with epidurals were far less likely to need additional pain relief (RR 0.10) and reported significantly higher satisfaction scores.
Yet epidurals remain one of the most misunderstood interventions in obstetrics. Myths about back pain, cesarean risk, and harm to babies persist across social media, birth classes, and even some provider conversations. Many of these beliefs are based on outdated studies using older, high-dose techniques that bear little resemblance to modern low-concentration epidural analgesia.
The evidence has moved. The conversation has not.
Here is what you need to know, and what to ask, before you are in the middle of a contraction.
The 17 Questions
1. Do epidurals increase my risk of a cesarean section?
What the evidence shows: No. The 2018 Cochrane review of 40 RCTs found no increased risk of cesarean delivery with epidural analgesia compared to opioid analgesia (1). A separate meta-analysis of early versus late epidural placement (9 RCTs, 15,752 women) found no difference in cesarean rates regardless of cervical dilation at the time of placement (RR 1.02, 95% CI 0.96-1.10) (2). A 2023 comprehensive review in the American Journal of Obstetrics and Gynecology confirmed that high-quality studies have “consistently shown no increased risk of cesarean delivery associated with epidural analgesia” (3). A 2025 retrospective study of 387 women in Saudi Arabia similarly found that while crude rates appeared higher with epidurals, multivariable analysis showed no significant effect (4).
The confusion persists because women with longer, more difficult labors are more likely to request epidurals. The epidural does not cause the cesarean. The difficult labor causes both.
What to do now: If a provider or family member tells you epidurals cause cesareans, ask them for the randomized trial that shows this. It does not exist in the modern literature. Make your pain relief decision based on your pain, not on fear of a surgical outcome the data does not support.
Below are 16 more evidence-based questions every pregnant person should be able to answer before labor. Each includes what the research shows and what to do with that information.
