

Reddit is where patients go at 2 a.m. when scared. I monitor dozens of communities for clinically meaningful posts: dangerous myths, gaps between belief and evidence, stories guidelines cannot capture. This series -- ObGyn Intelligence on Reddit -- dissects them against the literature, because ObGyns who ignore social media ignore the most unfiltered window into what patients think, fear, and do between appointments.
Summary
A first-time mother posted on r/pregnant describing 85 hours of active labor during which she was sent home from the emergency department twice after being told she was “1 cm and a wiggle” dilated. She appeared for a scheduled OB appointment -- which she almost skipped -- and her physician found her at 9.5 cm. She delivered the same day.
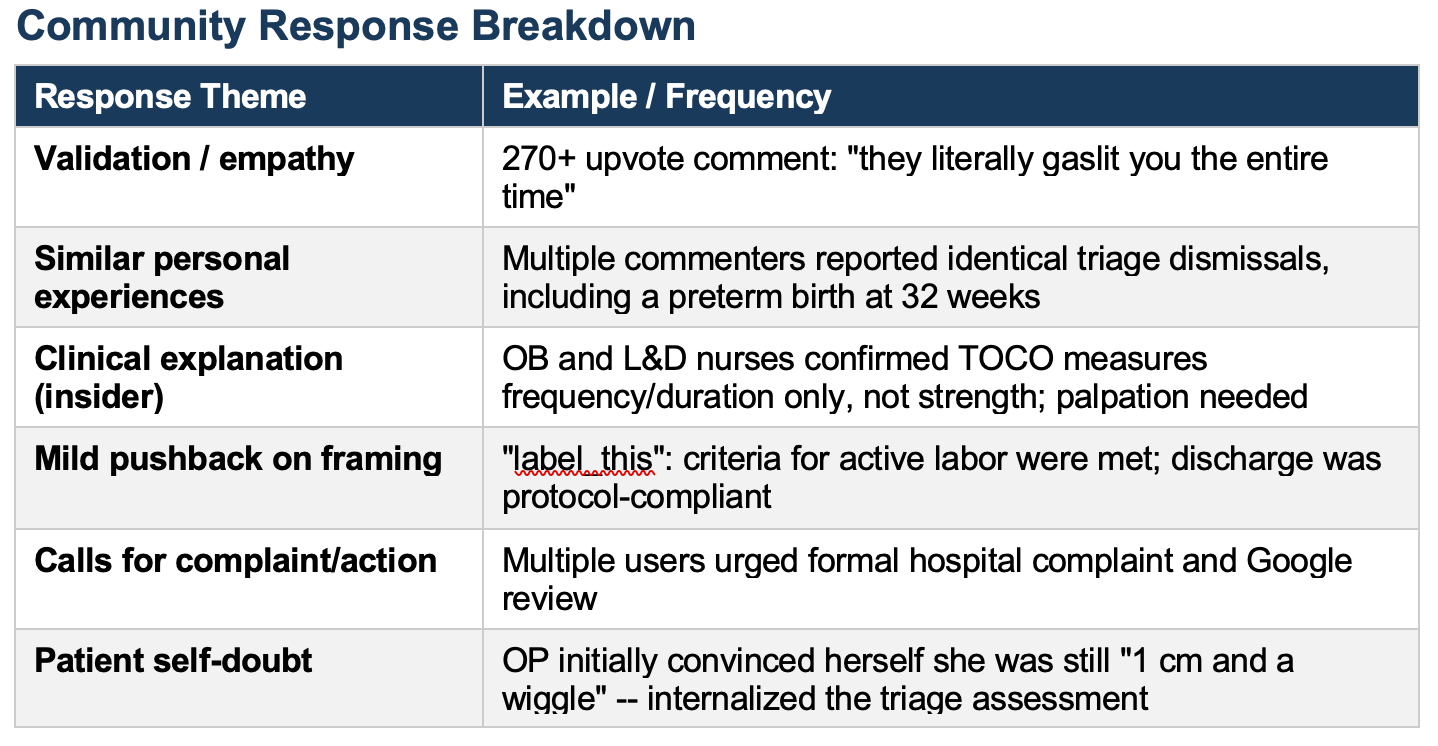
The post collected 429 upvotes and 53 comments. The community response was largely one of shared recognition: stories of similar dismissals poured in, including a commenter who delivered a preterm baby 24 hours after being told her contractions were not real. Several OB and L&D nurses in the comments acknowledged that TOCO monitor numbers do not measure contraction strength -- only frequency and duration -- while also noting that clinical staff routinely fail to explain this to patients.
The post is also a case study in how triage assessment errors compound. At the first visit, the cervix was described as posterior and unreachable. At the second visit, three nurses attempted cervical examination; the TOCO was mispositioned and registered near-zero values during contractions. The patient was sent home both times. She ultimately had to be persuaded by her OB to undergo the exam that revealed imminent delivery.
Evidence-Based Commentary
This post encodes four distinct clinical failures, each independently capable of causing harm, each compounded by the next. They deserve to be named precisely, not laundered as “prodromal labor” -- a term that appeared in the comments and that, while technically defensible, functions here as an explanation that excuses rather than examines.
But first of all, nobody asked if this was her first baby or not. Because that information is essential to try understanding what went on. Prior labors were fast, this will be again. First baby, and labor more likely longer.
The first failure is cervical examination technique. A posteriorly positioned cervix in early labor is not an anatomical surprise -- it is an expected finding. Standard obstetric teaching holds that a posterior cervix should be identified, documented with Bishop score components (position, consistency, effacement, dilation, station), and followed. The documented inability to reach the cervix at the first visit was not accompanied by any attempt to note cervical position, effacement, or station. “1 cm and a wiggle” is not a clinical finding; it is an estimate made under suboptimal conditions and communicated without a confidence interval. When three nurses are required to attempt the same exam at the second visit and arrive at the same number under worse monitoring conditions, that is a signal, not reassurance.
The second failure is TOCO interpretation and patient communication. The external tocodynamometer measures uterine wall movement, not intrauterine pressure. It is a measure of contraction frequency and duration -- not strength. This is not obscure physiology. It is in every obstetric nursing textbook. The nurse’s response at the second visit -- that contractions reaching 15 on the monitor “don’t really matter” -- is clinically accurate in isolation. TOCO numbers do not correlate with cervical change. But the framing weaponized accuracy against the patient. The appropriate response to a TOCO reading that contradicts clinical presentation is not “those numbers don’t matter” -- it is manual uterine palpation to assess contraction firmness, combined with re-examination. Neither occurred.
The third failure is the use of pain tolerance as a diagnostic criterion. “You’ll know when it’s real labor because it’s really painful” is not a triage standard. It is an assumption built on population averages that collapses in the face of individual variation, high pain tolerance, neurodivergent sensory processing, stoicism, or simply a labor pattern that progresses faster than the screaming-woman heuristic anticipates. Pain behavior correlates poorly with cervical dilation across individuals. A patient presenting repeatedly, over multiple days, with contractions 1.5-2 minutes apart has already provided the clinical signal. The decision to override that signal with behavioral expectations is not evidence-based practice.
The fourth failure is the most systematic: the absence of a safety netting plan. Both ER visits ended with discharge and no documented return precautions, no scheduled recheck at a defined time interval, and no instruction to call the OB before the next scheduled appointment. A patient in possible prodromal or early labor with a posteriorly positioned cervix should leave triage with explicit criteria: return if contractions reach X frequency, if membranes rupture, if fetal movement changes, or if pain becomes intolerable -- and with a low threshold for same-day OB contact. This patient almost did not go to her OB appointment because she had internalized the triage assessment. That near-miss is the consequence of inadequate safety netting, not inadequate patient judgment.
One comment in the thread deserves attention: a nurse wrote that TOCO numbers “truly don’t mean anything to us” -- and 103 people upvoted it. This sentiment is intended to be reassuring.
It functions instead as a description of a communication failure that predates this case and will outlast it. If a monitoring tool’s numbers do not mean anything to clinical staff, patients need to know that explicitly, in plain language, at the time the monitor is applied. What it actually measures. What it does not measure. What assessment will be used instead. That is informed consent for the monitoring process itself. Its absence here is not a minor oversight; it is why a woman spent 85 hours convinced that her body was lying to her.
What It Means
Labor triage errors are not rare. They are structurally predictable when assessment protocols rely on a single cervical measurement, TOCO numbers are allowed to override clinical judgment, and pain behavior is used as a proxy for dilation. This case is unusual in outcome -- 9.5 cm at an outpatient OB appointment -- but the pattern of dismissal it describes appears dozens of times in the comments alone. The comments are not outliers. They are prevalence data.
For clinicians, the actionable question is not whether this particular case could have been handled differently -- it obviously could. The question is what structural conditions allow this pattern to recur. The answer points to three specific gaps: incomplete cervical assessment documentation (Bishop score vs. a single number), no protocol for manual palpation when TOCO is unreliable, and no standardized safety netting language at labor triage discharge. None of these require new equipment. They require explicit expectations and the teaching to back them up.
The comment from the L&D nurse who said TOCO numbers “don’t really matter” is not wrong -- and it is also not good enough. Clinical staff knowing that TOCO is limited while patients believe it is the definitive labor meter is a communication gap with real consequences. Closing that gap is not the patient’s responsibility.
My Take
I have been in labor and delivery for five decades. I have seen this. The specific details change; the shape of it does not. A patient knows something is happening. She is told she does not. She eventually turns out to be right -- sometimes before a bad outcome, sometimes after.
What troubles me most about this case is not the triage failures, though they are real and correctable. It is the moment when this patient almost refused her OB appointment -- because she had been told enough times that her body was wrong that she believed it. She arrived at that appointment apologizing, promising her doctor she was not in active labor. She was 9.5 cm dilated and crying in pain.
The OB in this story did everything right. She insisted, with kindness, on a cervical exam. The look on her face when she found 9.5 cm is the image that stays with me. That look is the gap between what the system told this woman and what was actually happening inside her body. We close that gap not with better TOCO monitors but with better communication, better examination standards, and the professional honesty to tell patients exactly what our tools can and cannot measure -- before they spend 85 hours doubting themselves.