
Breaking: Dry-Erase Board Eliminates Racial Disparities in Obstetrics. Harvard Researchers Cautiously Optimistic. Whiteboard Unavailable for Comment.

We Put a Whiteboard in the Labor Room. Racial Disparities Fell. Coincidence? Probably. But We Made a Graph.

A whiteboard is not a patient safety intervention. It is a whiteboard.
And if you make it black, it’s a blackboard.
This is actually NOT an April fool joke.
I want to start there, because somewhere between Harvard and the press release, this distinction got lost.
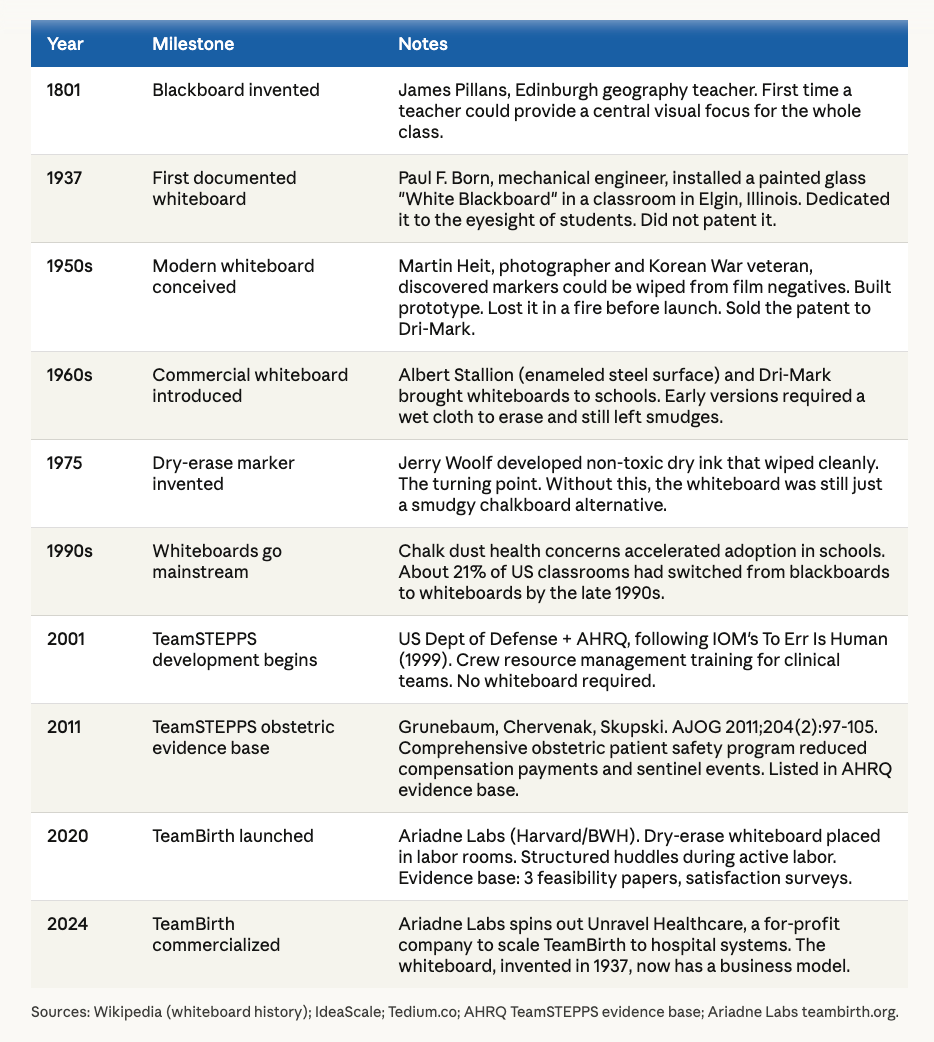
Ariadne Labs, a joint center of Brigham and Women’s Hospital and the Harvard T.H. Chan School of Public Health, has built something called TeamBirth. It involves structured huddles at the bedside during labor, documented on a patient-facing dry-erase board mounted in the labor room. The goal is shared decision-making. The pitch is patient safety. The evidence, as I will explain, is satisfaction surveys. And the business model is now, formally, a for-profit company.
I do not doubt the sincerity of the people behind it. I question the claim that this is new, that it is evidence-based, and that it solves the problem it claims to solve.
In 2026, at a moment when artificial intelligence can read a fetal heart rate tracing, predict postpartum hemorrhage before it happens, draft a discharge summary, and pass the obstetrics board exam, Ariadne Labs — a joint center of Harvard and Brigham and Women's Hospital — has determined that the future of patient safety in labor and delivery is a dry-erase board on the wall.
Not an app.
Not an integrated dashboard pulling from the EHR.
Not an AI-assisted decision support tool. A whiteboard.
With markers.
That someone has to walk over to and write on by hand.
During active labor.
Most labor and delivery units, including our own, replaced physical boards with electronic L&D tracking systems well over a decade ago — systems that update in real time, are visible from any workstation, integrate with monitoring, flag deteriorating patients, and do not require a nurse to find a working marker.
We gave up the whiteboard because it was inefficient, error-prone, and invisible the moment anyone walked out of the room.
And because we often ran out of markers.
Ariadne Labs has brought it back, given it a logo, written three papers about it, and spun out a for-profit company to sell it to hospitals. The whiteboard was invented in 1937. It is nice to see it getting a second career.
The Adriadne site is full of AI generated graphs and images.
Like this here:

Or this:
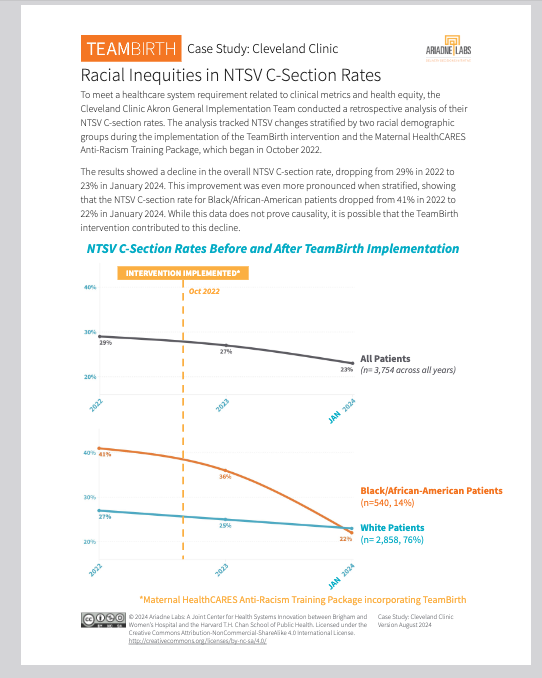
What Ariadne is claiming in this graph above.
A retrospective analysis at one hospital — Cleveland Clinic Akron General — tracking NTSV cesarean rates before and after TeamBirth implementation in October 2022. Overall rate dropped from 29% to 23%. Black/African-American patients dropped from 41% to 22%.
They acknowledge it does not prove causality.
What is wrong with this, systematically
No control group. There is no concurrent comparison hospital without TeamBirth. The secular trend in NTSV cesarean rates was already declining nationally during this period. Without a control, you cannot separate TeamBirth’s effect from background drift, regression to the mean, or any other concurrent intervention — including the Maternal HealthCARES Anti-Racism Training Package, which they note was implemented simultaneously. That alone is a fatal confound.
Two interventions, one line. The footnote quietly acknowledges that TeamBirth and the Maternal HealthCARES Anti-Racism Training Package were implemented together in October 2022. There is no attempt to disentangle them. The graph attributes the decline to TeamBirth in the title, then the text says “possible.” That is not scientific caution. That is having it both ways.
N=540 for Black patients over all years. The subgroup driving the most dramatic finding — a 19 percentage point drop — has 540 patients across multiple years. That is a small, single-site convenience sample. The confidence intervals are not shown. The statistical significance is not reported. A 19-point swing in a small sample at a single motivated pilot site is not evidence of an intervention effect. It is noise dressed in orange font.
Retrospective design with no pre-specified hypothesis. This is a post-hoc analysis of administrative data. The outcome was chosen after the fact. The time points were chosen after the fact. This is the definition of a study designed to confirm rather than test.
“It is possible that TeamBirth contributed.” This phrase has a precise scientific meaning: we have no evidence either way, but we cannot rule it out.
It is the epistemological equivalent of saying it is possible that the new parking lot also reduced cesarean rates.
Everything is possible.
Nothing is demonstrated.
What would an honest graph look like
It would show: the national NTSV trend over the same period, a concurrent control hospital, confidence intervals on every data point, and separate lines for TeamBirth alone versus TeamBirth plus anti-racism training. It would be submitted to a peer-reviewed journal and survive external review before appearing in a case study with a TeamBirth logo at the top.
The bottom line
This is a marketing document formatted as evidence. The disclaimer — “this data does not prove causality” — is not scientific humility. It is legal protection. They are presenting a dramatic graph, attributing it by implication to their product, and then retreating behind a single qualifying sentence when pressed.
That is not how science works. That is how whiteboards get sold.
We did this twenty years ago
In the early 2000s, following the Institute of Medicine’s landmark report To Err Is Human, the US Department of Defense and the Agency for Healthcare Research and Quality developed TeamSTEPPS -- Team Strategies and Tools to Enhance Performance and Patient Safety. It was modeled on aviation crew resource management. It trained the clinicians: communication frameworks, situational awareness, mutual support, leadership under pressure, simulation drills, structured debriefing after adverse events.
The evidence base that followed was real.
A Cochrane review of simulation-based obstetric team training -- much of it TeamSTEPPS-derived -- included 8 randomized controlled trials and more than 200,000 pregnancies. It found that simulation-based team training probably reduces the cesarean rate (RR 0.79, 95% CI 0.67-0.93) and probably reduces shoulder dystocia trauma (RR 0.50, 95% CI 0.25-0.99). Those are clinical outcomes. Babies. Mothers. Numbers that matter.
Our own published Research
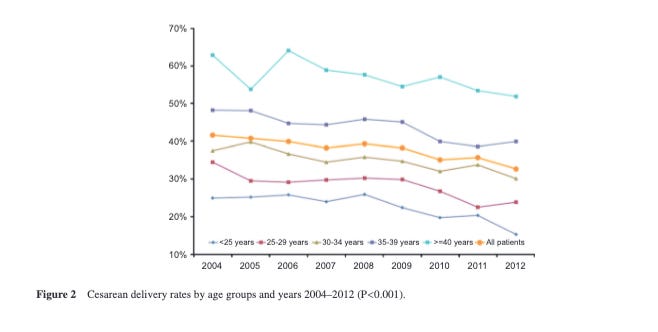
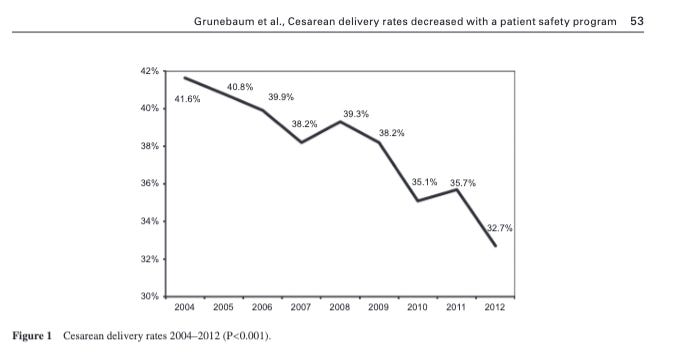
Our own work published in AJOG in 2011 -- showed that a comprehensive obstetric patient safety program reduced compensation payments and sentinel events. That paper is listed in the AHRQ TeamSTEPPS evidence base. Not because we asked to be there, but because the data supported inclusion.
We also showed that we reduced cesarean delivery rates.
Not for 500 patients but 45,655 over 8 years.
TeamSTEPPS is also free. The full curriculum is available from AHRQ at no charge. No spinout required.
What TeamBirth actually is
TeamBirth places a dry-erase whiteboard in the labor room. A clinical team member fills it out at admission. It is updated during huddles throughout labor. The patient is invited to participate. Everyone writes things down. This is the intervention.
I do not say that dismissively.
Including the patient in bedside discussions is better than excluding her.
Written documentation of preferences is better than verbal-only. Structured huddles beat hallway decisions. These are improvements over a low baseline.
But the baseline was low precisely because we stopped doing TeamSTEPPS properly. The answer to that problem is not a whiteboard with a Harvard logo. It is to return to the training that actually worked.
The evidence problem
Ariadne Labs reports that 97% of TeamBirth patients felt they had the role they wanted in their care, and 93% of clinicians felt it improved communication. These numbers come from post-delivery satisfaction surveys. They measure whether patients felt involved. They do not measure whether patients understood the absolute risks of the interventions they agreed to. Feeling heard and being genuinely informed are different things.
The only clinical metric cited is a nearly 4% reduction in the primary cesarean rate at the pilot site, South Shore Hospital. One hospital. No randomized control group. No adjustment for secular trends. No GRADE assessment. In the evidence hierarchy, this is a case report with a whiteboard.
TeamBirth has published three papers in Birth: Issues in Perinatal Care -- a feasibility study, an acceptability and safety study, and a qualitative implementation study. The team itself concluded that future research should explore acceptability in less engaged hospitals. That is honest. But it is also the language of a pilot program, not an industry standard ready for 130 hospitals.
TeamSTEPPS: 8 RCTs. 200,000+ births. Clinical outcomes. Free.
TeamBirth: 3 feasibility papers. 4 pilot hospitals. Satisfaction surveys. Now sold through a for-profit company.
I am not saying these facts are decisive. I am saying they should appear prominently in every presentation of TeamBirth to hospital administrators.
The commercial turn
In 2024, Ariadne Labs spun out Unravel Healthcare, a for-profit company dedicated to scaling TeamBirth to health systems. Ariadne Labs -- a nonprofit academic center -- has created a commercial vehicle to sell its own product while simultaneously publishing the research that supports that product.
This is a conflict of interest. It should be disclosed in every paper, every press release, and every pitch to a hospital. I have not seen it disclosed prominently in any of them.
The core materials remain free, I am told. The implementation support -- the part that actually produces the culture change TeamBirth requires -- now has a price.
My take
Good communication during labor is better than bad communication.
A patient who feels included is better than one who is ignored.
On these points, TeamBirth and I (and we all) agree completely.
But the obstetric safety problem was never caused by the absence of a whiteboard. It was caused by hierarchical communication failures, inadequate simulation training, physicians and nurses who had never practiced managing a shoulder dystocia together before one appeared, and institutions that measured satisfaction rather than outcomes.
TeamSTEPPS addressed those root causes. It trained the team. It measured what happened to patients. It was available to every hospital in America for free, backed by two decades of RCT evidence, and endorsed by AHRQ and the Department of Defense.
TeamBirth put a whiteboard in the room and surveyed patients afterward about how they felt.
One of these is patient safety. The other is patient experience. Both matter. But they are not the same thing, and presenting one as the other is a disservice to the hospitals being asked to implement it, the clinicians being asked to change their practice, and the patients whose outcomes hang in the balance.
We already had the tool. It worked. The question worth asking is why we stopped using it -- and whether a new brand with a dry-erase board is really the answer.