
Coffee and Reproductive Health: What the Evidence Actually Shows
From fertility to breastfeeding, the data tells a more nuanced story than the headlines suggest.

I'll confess upfront: I love coffee. After falling down the YouTube rabbit hole of James Hoffmann's methodical brewing experiments, and subsequently acquiring more coffee gadgets than any kitchen needs (my partner is very accepting), I've settled on the AeroPress as my daily driver. So when patients ask me about caffeine in pregnancy, I'm not speaking as someone who finds the topic abstract. And according to the New York Times drinking coffee may even boost your mood.
Two-thirds of American adults drink coffee daily. For women trying to conceive, pregnant, or nursing a baby, the question inevitably arises: Should I give it up?
The answer depends on which phase of reproduction you’re in—and how you weigh imperfect evidence.
The Problem With Studying Coffee in Pregnancy
Before diving into the data, you need to understand a critical methodological issue that haunts this entire field: reverse causation.
Nausea and food aversions are more common in healthy pregnancies. Women experiencing robust pregnancy symptoms—the very ones with viable pregnancies—naturally reduce their caffeine intake because coffee suddenly tastes terrible or makes them queasy. Women whose pregnancies are already failing often continue drinking coffee normally because they don’t feel as sick.
This creates a confounding nightmare. Does caffeine cause miscarriage? Or do women destined to miscarry simply drink more coffee because their pregnancies never triggered the normal aversion response?
Researchers have tried to control for this by measuring caffeine before nausea onset, stratifying by symptom presence, and using biomarkers instead of self-report. The results remain contested. Keep this limitation in mind as we review the evidence.
Fertility: Not Much Signal
The good news for coffee lovers trying to conceive: the evidence of harm is weak.
A systematic review and dose-response meta-analysis found no clear association between coffee or caffeine consumption and time to pregnancy among couples trying naturally or through fertility treatment. Women drinking several cups daily conceived at similar rates to abstainers.
A separate systematic review including four controlled studies found that low, medium, and high doses of caffeine did not significantly increase infertility risk. The quality of evidence was rated low, but the point estimates showed no meaningful effect.
One older study from the 1980s suggested fecundability was halved by just one cup daily, but subsequent larger studies haven’t replicated this finding.
Bottom line for fertility: If you’re trying to conceive, moderate coffee consumption probably isn’t delaying your pregnancy.
Pregnancy: This Is Where It Gets Complicated
ACOG’s position hasn’t changed since 2010: moderate caffeine consumption (less than 200 mg per day, roughly one 12-ounce cup of coffee) “does not appear to be a major contributing factor in miscarriage or preterm birth.”
The data supporting caution at higher intakes, however, is more robust.
Pregnancy Loss
Multiple meta-analyses converge on similar findings:
Each 100 mg/day increment in caffeine (about one cup of coffee) is associated with a 7-14% higher risk of pregnancy loss
Risk becomes statistically significant at high intakes (>300-350 mg/day)
The dose-response relationship is linear—no clear threshold below which risk disappears
A 2022 GRADE-assessed meta-analysis of 34 studies found increased pregnancy loss risk for coffee consumption both before pregnancy (pooled effect 1.21) and during pregnancy (1.26).
The most recent nuMoM2b cohort study (2024) of over 7,300 nulliparous women found no association between periconceptual caffeine intake under 200 mg/day and adverse pregnancy outcomes—including no increased odds of spontaneous pregnancy loss. This study measured intake before women knew they were pregnant, partially addressing the reverse causation problem.
Fetal Growth
The association with growth restriction is more consistent than the miscarriage data.
Meta-analyses report that each 100 mg/day caffeine increment is associated with:
7-13% higher risk of low birth weight
10% higher risk of small-for-gestational-age
A 2024 Finnish cohort found that even moderate caffeine intake during the first trimester (within the “safe” 200 mg limit) was associated with increased SGA risk—with odds ratios as high as 2.44 for the highest consumption tertile.
The James Controversy
In 2020, psychologist Jack James published a narrative review in BMJ Evidence-Based Medicine concluding there is “no safe level” of caffeine in pregnancy. He called for “radical revision” of guidelines, recommending complete abstinence.
ACOG responded within days: “Our guidance remains that moderate caffeine consumption, less than 200 mg per day, does not appear to be a major contributing factor in miscarriage or preterm birth.”
James’s review was provocative but not definitive. He relied heavily on observational data, dismissed the reverse-causation concern more readily than most researchers would, and is a psychologist—not an obstetrician or epidemiologist—working at an institution without a medical school.
The professional societies held their ground. The data hasn’t changed enough to alter recommendations.
Here’s a paragraph you can insert (probably best placed just before or after the “Putting It Together” section):
What Is “A Cup” Anyway?
When guidelines say “200 mg of caffeine” or “one to two cups,” they’re using terms that mean different things to different people. A “cup” in research typically means 8 ounces (240 mL)—not the 12-ounce “tall” or 16-ounce “grande” you get at Starbucks, and certainly not the 20-ounce venti. Your home mug likely holds 12-16 ounces.
Caffeine content varies dramatically by preparation method:
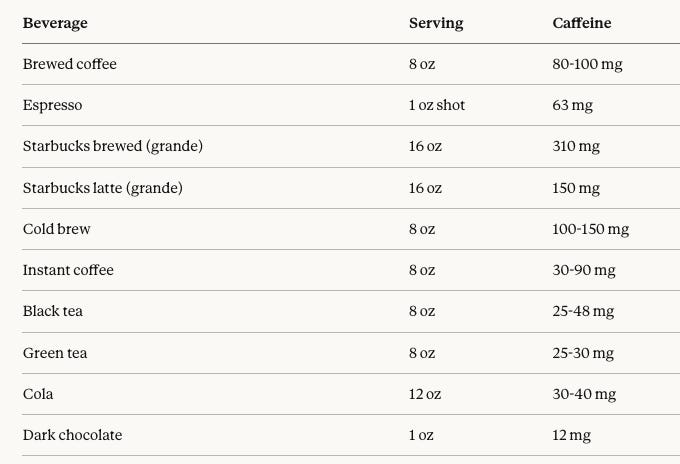
The practical point: a single Starbucks grande brewed coffee already exceeds the 200 mg pregnancy limit. A grande latte (two shots of espresso diluted with steamed milk) is actually the safer choice at 150 mg. If you’re tracking intake, know your actual serving sizes and preparation methods—not the idealized “cup” in the guidelines.
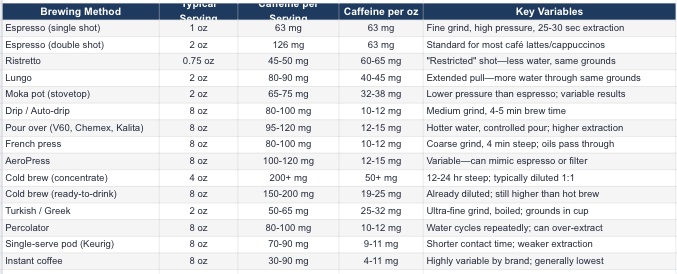
Caffeine by Brewing Method
Not all coffee is created equal. Extraction depends on grind size, water temperature, contact time, and pressure. Here’s what you’re actually getting:
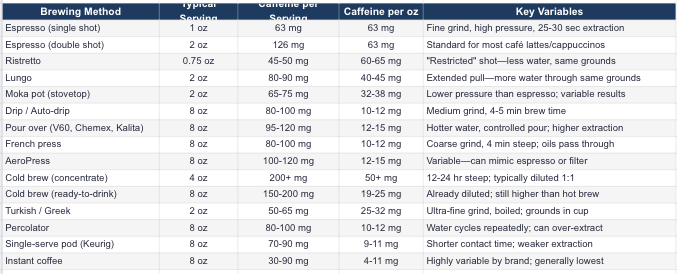
What Affects Caffeine Extraction
More caffeine: Finer grind, longer contact time, hotter water, higher coffee-to-water ratio, Robusta beans
Less caffeine: Coarser grind, shorter contact time, cooler water, lower ratio, Arabica beans
Roast level: Contrary to popular belief, light and dark roasts have similar caffeine by weight. Dark roasts taste “stronger” but aren’t more caffeinated.
Practical Translation for Pregnancy
The 200 mg limit means roughly:
One double-shot latte (126 mg) leaves room for a small tea later
One 12-oz drip coffee (120-150 mg) is close to the limit
One Starbucks grande brewed (310 mg) exceeds it
One cold brew (150-200 mg) may already be at or over limit
Two single espresso shots throughout the day (126 mg total) is fine
If you drink pour-over or French press at home, measure your actual cup—most mugs hold 12-16 oz, not 8.
The Biology Is Plausible
Caffeine crosses the placenta freely. Fetal serum concentrations equal maternal levels. The developing fetus lacks the cytochrome P450 enzymes (CYP1A2) needed to metabolize caffeine, so exposure persists.
During pregnancy, the mother’s caffeine metabolism slows dramatically. Half-life extends from 4-5 hours in the first trimester to about 15 hours by the third trimester. A morning cup lingers much longer than it did before conception.
Proposed mechanisms for harm include:
Catecholamine release causing placental vasoconstriction and fetal hypoxia
Elevated cyclic AMP affecting cellular growth
Direct effects on developing neural tissue (caffeine metabolites accumulate in fetal brain)
Breastfeeding: A Different Risk Profile
Postpartum, the equation shifts.
Only 0.06-1.5% of ingested caffeine appears in breast milk. Peak levels occur one to two hours after consumption. For a mother drinking 300 mg of caffeine, the infant receives somewhere between 0.18 and 4.5 mg—well below therapeutic doses.
For context: premature infants in the NICU routinely receive 5 mg/kg of caffeine as treatment for apnea of prematurity.
The catch: newborns metabolize caffeine extremely slowly. The half-life in a term newborn is about 80 hours—compared to 3-7 hours in adults. In preterm infants, it can exceed 100 hours. Caffeine accumulates.
By 3-5 months, infant caffeine metabolism improves dramatically, with half-life dropping to roughly 14 hours.
What the Guidelines Say
The CDC considers 300 mg or less per day “generally safe” for breastfeeding mothers. EFSA (European Food Safety Authority) sets the limit at 200 mg. Both acknowledge individual variation.
Signs of caffeine sensitivity in breastfed infants include irritability, fussiness, jitteriness, and sleep disturbance. If your baby shows these signs—especially if premature or under three months—reducing intake is reasonable.
One study found that intakes above 450 mg/day were associated with lower iron levels in breast milk. Given the importance of iron in infant neurodevelopment, heavy consumers should be aware.
Energy Drinks: A Caution
Energy drinks present a different risk profile than coffee. Variable caffeine content, added stimulants (guarana, taurine), and inadequate safety data for breastfeeding make them a poor choice. Australian food standards require warning labels stating they’re unsuitable for pregnant and breastfeeding women. This is reasonable advice.
Putting It Together: Evidence-Based Recommendations
Trying to conceive: Moderate coffee consumption (2-3 cups/day) likely has no meaningful effect on fertility. Don’t stress about your morning cup.
Pregnant: Limit to 200 mg/day or less. This is the ACOG recommendation and remains defensible given current evidence. The association with growth restriction at higher intakes is concerning even if the miscarriage data is confounded. Less is probably better, but complete abstinence isn’t clearly necessary based on available evidence.
Breastfeeding: 200-300 mg/day is generally safe. Preterm infants and newborns under 3 months are more sensitive—err on the lower end. Watch your baby for irritability or sleep disruption. By 4-6 months, typical consumption presents minimal concern.
What We Still Don’t Know
The field lacks adequately powered randomized trials—and likely always will, given the ethical impossibility of randomizing pregnant women to high caffeine exposure. We’re left interpreting observational data with all its limitations.
The reverse causation problem remains partially unresolved. Even sophisticated statistical adjustments may not fully capture the biology of pregnancy viability affecting caffeine intake.
Individual genetic variation in caffeine metabolism (CYP1A2 polymorphisms) likely moderates risk, but we don’t yet have clinically useful genetic testing to guide recommendations.
There is an important point about coffee: the food industry has turned a genuinely healthy beverage into vehicles for delivering massive amounts of sugar. A Dunkin’ French vanilla swirl frozen coffee delivers 132 grams of sugar—more than three times a typical soda.
If you’re going to drink coffee during pregnancy or breastfeeding, drink actual coffee. Not a milkshake with espresso somewhere inside.