
“Drink Your Water” ObI | The Digital Waiting Room
Reddit is where patients go at 2 a.m. when scared. I monitor dozens of communities for clinically meaningful posts: dangerous myths, gaps between belief and evidence, stories guidelines cannot capture

Reddit is where patients go at 2 a.m. when scared. I monitor dozens of communities for clinically meaningful posts: dangerous myths, gaps between belief and evidence, stories guidelines cannot capture. This series -- ObGyn Intelligence on Reddit -- dissects them against the literature, because ObGyns who ignore social media ignore the most unfiltered window into what patients think, fear, and do between appointments.
Summary
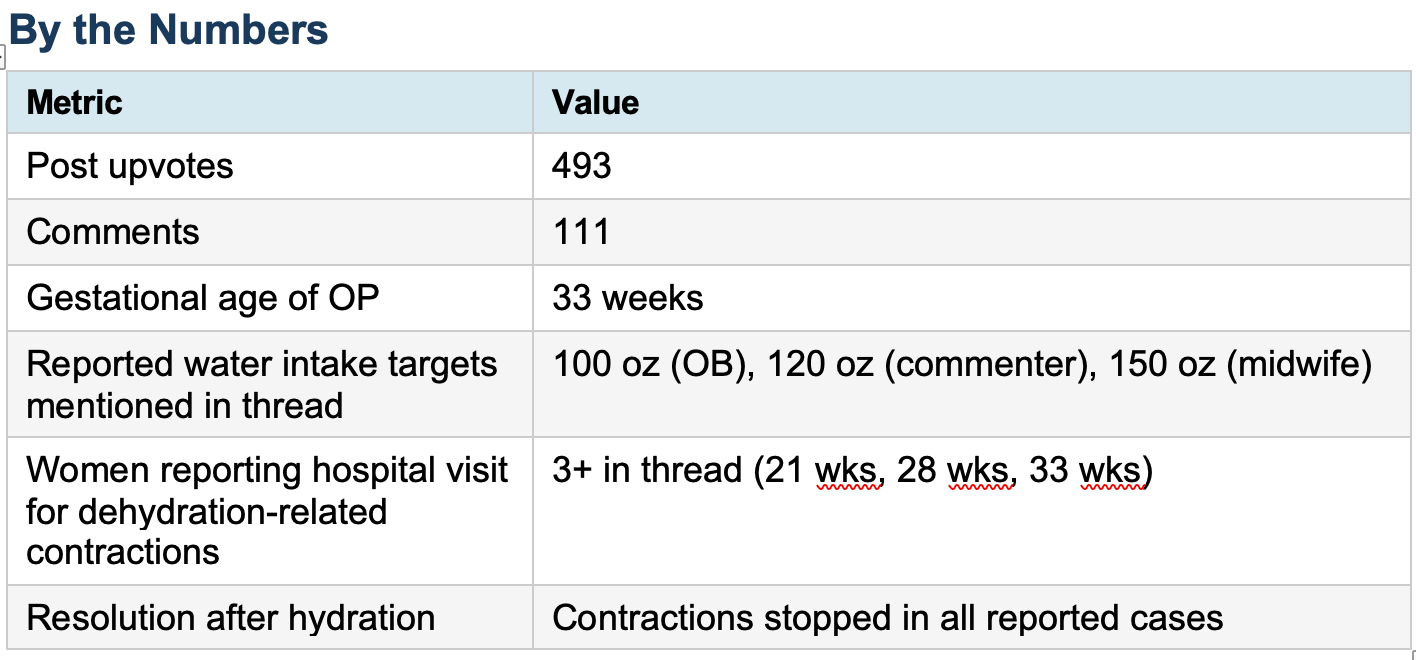
A 33-week pregnant woman posted to r/pregnant after an unplanned hospital visit. She had spotting and silent contractions. The doctors gave her water and a snack. Everything stopped. She was sent home fine. Her post -- written in all caps -- went viral within hours: 493 upvotes, 111 comments. The message was simple: she thought she was hydrated because she was urinating frequently. She was wrong. Frequent urination in pregnancy is caused by fetal pressure on the bladder, not by adequate fluid intake. The two are not the same. Her uterus was cramping from dehydration. The thread quickly filled with identical stories: women at 21, 28, and 35 weeks who had gone to labor and delivery for the same reason and were sent home with water.
Evidence-Based Commentary
Dehydration-triggered uterine contractions are not folklore. The mechanism is physiologically real. Myometrial smooth muscle, like all muscle, is sensitive to electrolyte balance and intravascular volume. Dehydration raises plasma osmolality, triggers antidiuretic hormone (ADH) release, and -- crucially -- stimulates oxytocin co-secretion from the posterior pituitary. Oxytocin drives uterine contractions. This is not a controversial pathway. It is well documented.
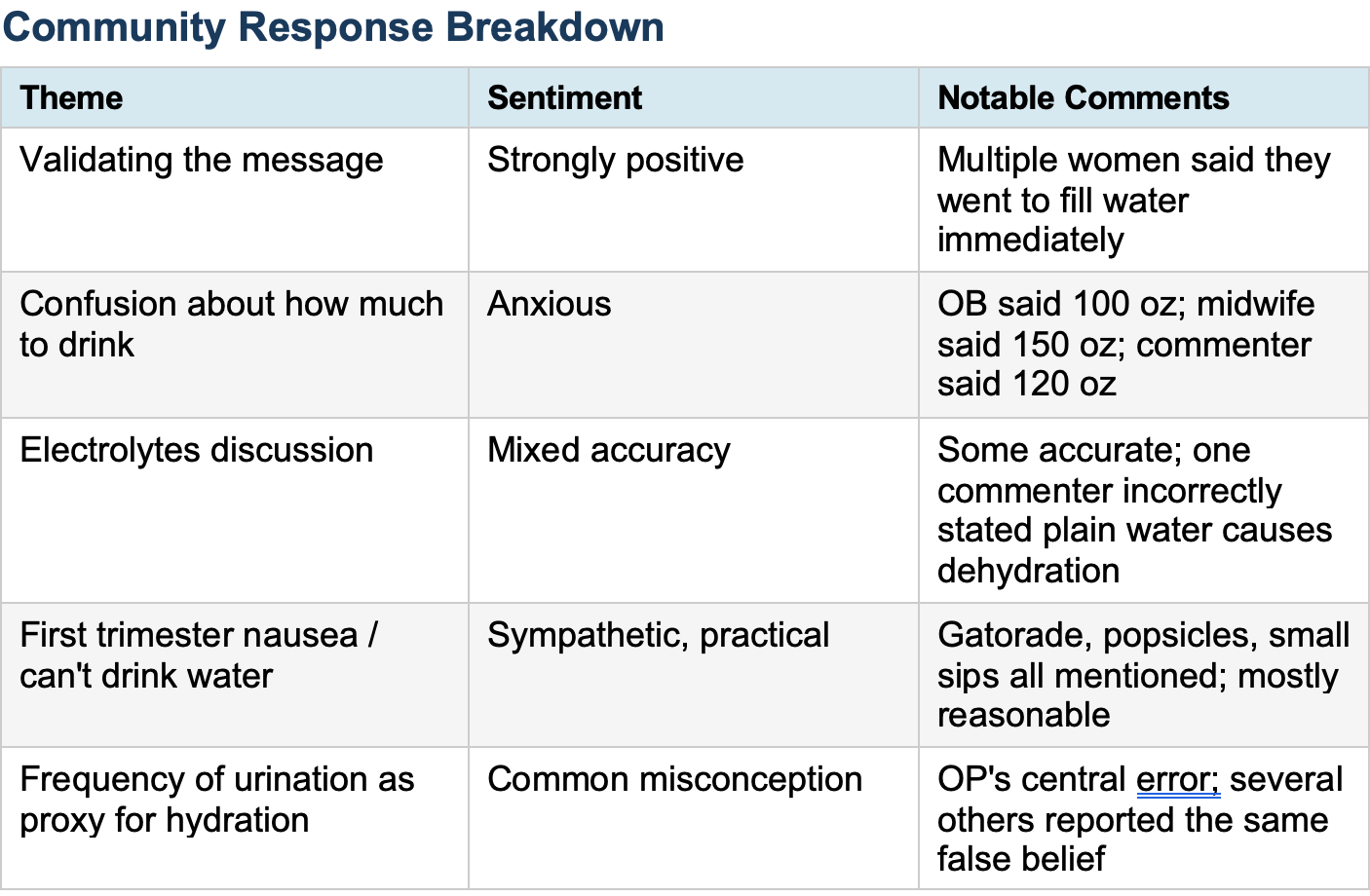
The misconception at the center of this post -- that frequent urination equals adequate hydration -- is one of the most common errors I hear from pregnant patients. It needs to be corrected at every prenatal visit. In pregnancy, urinary frequency is driven primarily by the growing uterus compressing the bladder, reducing its functional capacity. A woman can void every 45 minutes and still be volume-depleted if her fluid intake is insufficient. Urine color is a better -- though imperfect -- clinical proxy: pale yellow suggests adequate hydration; dark yellow or amber signals the opposite. One commenter in the thread noticed her urine looked like apple juice at the time of delivery despite hourly voiding. That is not an edge case. That is a predictable consequence of confusing frequency with volume.
How much fluid does a pregnant woman actually need? The honest answer is: it depends, and the guidance in this thread ranged from 100 to 150 ounces per day. ACOG does not issue a specific numeric daily fluid target for uncomplicated pregnancy. The Institute of Medicine (now the National Academy of Medicine) recommends approximately 2.3 liters (roughly 78 ounces) of total water per day from all sources, with higher needs in hot climates, with physical activity, or in the setting of vomiting. A midwife recommending 150 ounces daily is operating well outside evidence-based guidelines -- and for a patient with cardiac or renal compromise, that level of intake could be genuinely dangerous. Blanket high-number targets are not evidence-based. Context matters.
One commenter stated plainly that plain water causes dehydration and that electrolytes must always accompany fluid intake. This is wrong. Electrolyte supplementation is beneficial in specific clinical settings: hyperemesis gravidarum, excessive sweating, or prolonged exertion in heat. For a healthy pregnant woman sitting at home, plain water is appropriate hydration. Overuse of electrolyte packets -- particularly high-sodium formulations -- can contribute to edema and, in susceptible patients, worsen hypertensive disorders. The endorsement of commercial electrolyte products as routine pregnancy supplements, driven partly by influencer marketing, is not supported by evidence.
The thread also surfaced a real clinical challenge: first-trimester nausea that makes adequate fluid intake genuinely difficult. The community’s responses here were largely practical and reasonable -- popsicles, diluted juice, small frequent sips, Pedialyte. From a clinical standpoint, the key threshold is this: if a patient cannot keep any fluids down for more than 24 hours, or if she shows signs of ketonuria, orthostatic hypotension, or weight loss, she needs IV hydration and evaluation for hyperemesis gravidarum -- not Reddit advice. The community is rightly encouraging each other to drink; the limits of that encouragement are what providers need to establish clearly.
What It Means
This thread represents a real and preventable gap in prenatal education. Women are reaching 33 weeks of pregnancy -- past viability, well into the third trimester -- without understanding that frequent urination does not mean adequate hydration. That is a failure of prenatal counseling, not a failure of the patient. The information she needed was simple, practical, and potentially saved her from a much more complicated outcome. If this woman had been farther from a hospital, if she had dismissed the spotting, if the contractions had continued -- the stakes escalate quickly.
Obstetric providers should address hydration directly at every visit in the third trimester: not a pamphlet, not a general reminder, but a specific conversation about urine color as a monitoring tool, the inadequacy of urinary frequency as a hydration proxy, and individualized fluid targets based on the patient’s size, activity level, climate, and clinical picture.
My Take
I have watched this happen on labor and delivery more times than I can count. A patient arrives with contractions she cannot feel, a fetal heart rate that looks fine, and a urine sample that tells the whole story. We give her two liters of IV saline. The contractions stop. She goes home. The visit should never have happened.
What strikes me about this thread is not the original post -- that story is familiar. What strikes me is the noise. Women are getting conflicting fluid targets from their providers: 100 ounces from one OB, 150 from a midwife, 120 from the internet. Nobody is explaining why. Nobody is giving them a tool they can use at home -- like urine color -- to actually monitor themselves. Instead, they are collecting numbers and doing the math wrong.
And underneath all of it: a perfectly correctable misconception. Frequent urination does not mean you are hydrated. In pregnancy, it means you have a baby sitting on your bladder. Every prenatal provider should say that sentence out loud, at every third-trimester visit, until it sticks. It takes ten seconds. It might prevent a hospital admission.