
Improving Communication in Pregnancy: A Neurodivergent-Responsive Approach
Published in the American Journal of Obstetrics & Gynecology

Improving Communication in Pregnancy: A Neurodivergent-Responsive Approach, published in the American Journal of Obstetrics & Gynecology in 2026 by Grünebaum et al., argues that obstetric care must recognize communication and sensory processing differences before they become barriers during labor, consent, delivery, and postpartum care.
The paper focuses on neurodivergent pregnant women, including those with autism, ADHD, sensory processing differences, learning disorders, developmental coordination disorder, or Tourette syndrome. Its central point is simple: the goal is not to diagnose neurodivergence in the obstetric office. The goal is to identify how a patient receives information, processes stress, tolerates touch, and participates in time-sensitive decisions.
The paper emphasizes that pregnancy and labor are sensory-intensive experiences. Fetal monitoring, cervical exams, venipuncture, ultrasound, alarms, bright lights, repeated touch, urgent explanations, and unfamiliar staff can overwhelm patients whose processing needs are not recognized. What may look like anxiety, refusal, distrust, “noncooperation,” or poor motivation may instead reflect a mismatch between standard obstetric communication and the patient’s processing style.
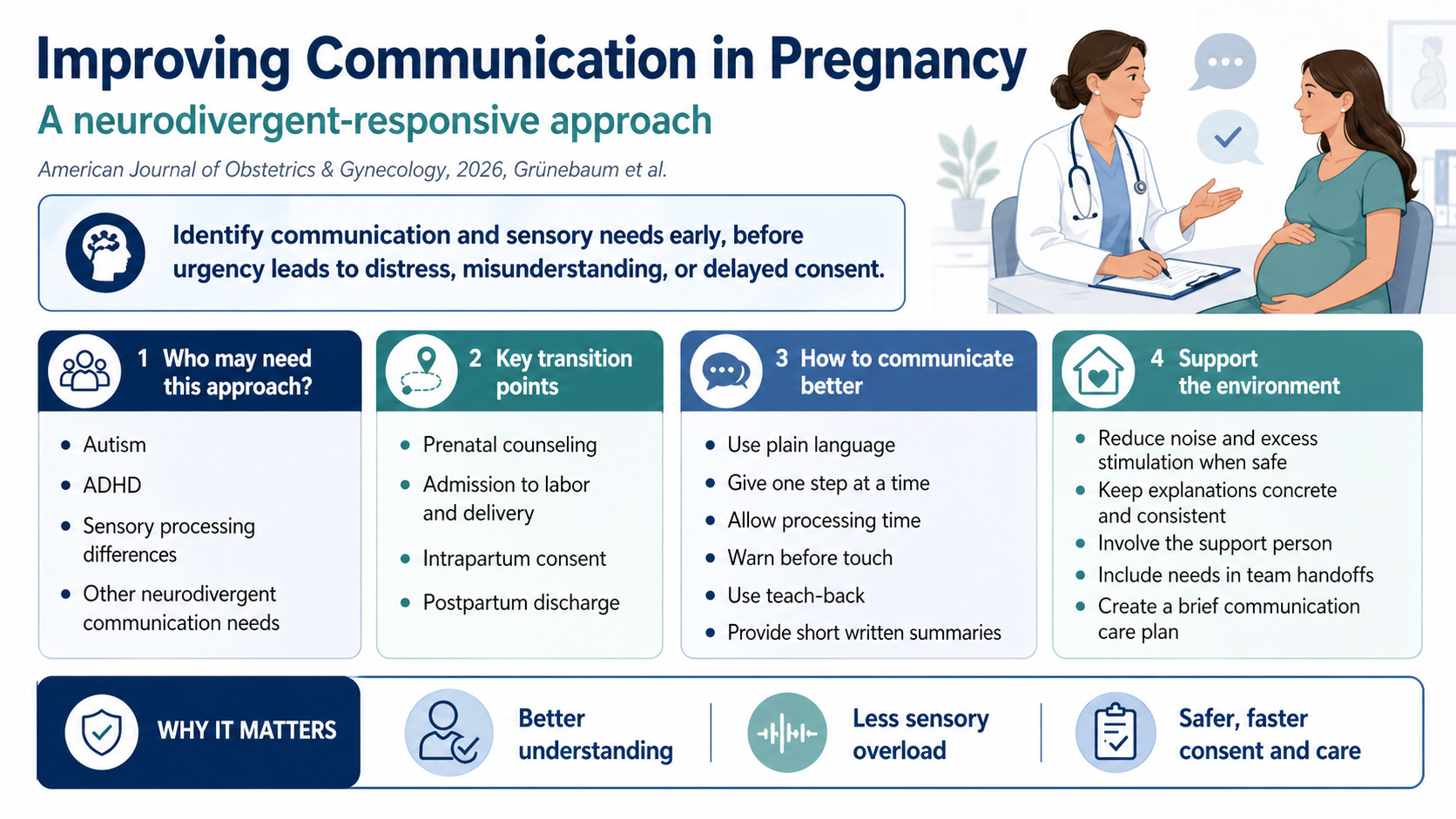
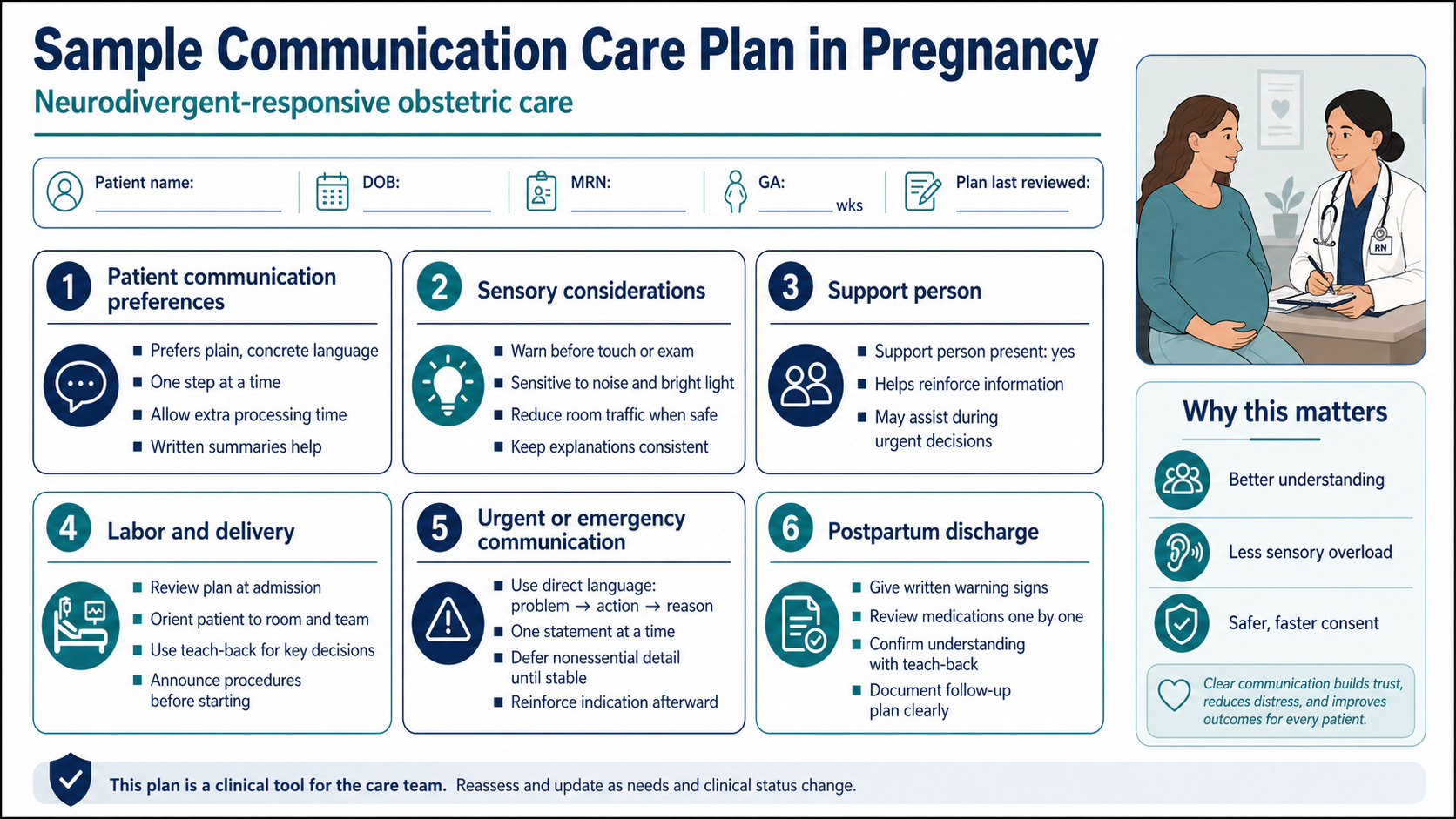
The proposed solution is practical. Clinicians should ask early about communication preferences, written versus verbal instructions, sensory triggers, processing time, warning before touch, and the role of a support person.
These needs should be documented in a brief communication care plan, visible to the labor and delivery team, and included in handoffs. During labor, clinicians should use plain language, give one instruction at a time, allow processing time, warn before examinations, reduce unnecessary stimulation when safe, involve the support person, and use teach-back to confirm understanding.
This approach is especially important during urgent intrapartum decisions, when complex explanations may delay consent or worsen distress. In emergencies, the paper recommends direct, concrete statements: problem, action, reason. Details can be reinforced afterward with written summaries.
The evidence base remains limited and is drawn largely from qualitative studies and patient-reported experiences rather than randomized obstetric outcome trials.
Still, the clinical logic is strong. Better communication is not a separate program. It is basic obstetric safety adapted to patients whose needs have too often been missed.