
“Is This Hospital a Good Place to Give Birth?”

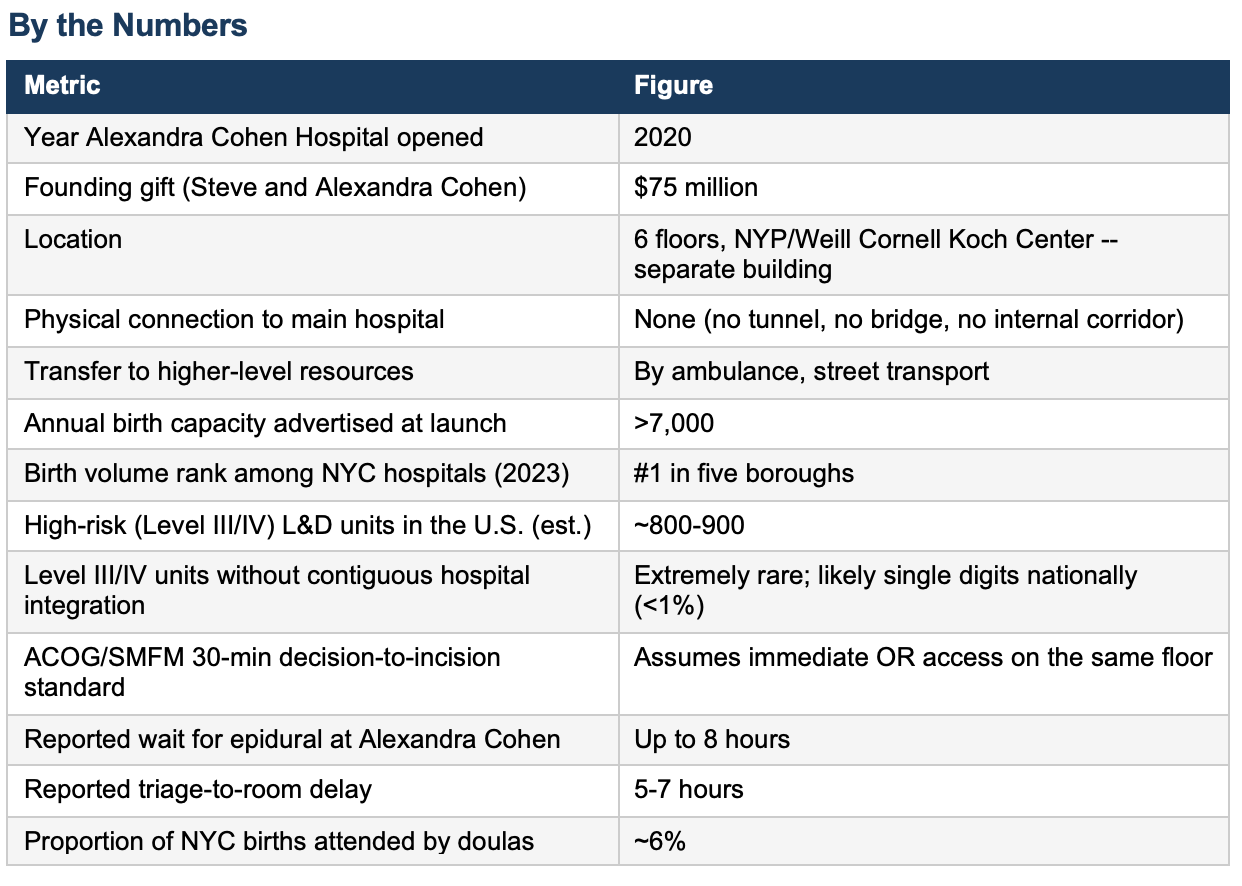
A March 2026 investigative report in The Cut (New York Magazine, author Irin Carmon) examined the Alexandra Cohen Hospital for Women and Newborns, the busiest birth hospital inside NYP/Weill Cornell’s David H. Koch Center on the Upper East Side, across the street from the main hospital.
Track your pregnancy week by week — your free pregnancy guide from ObGyn Intelligence.
No tunnel.
No bridge.
No direct hospital access.
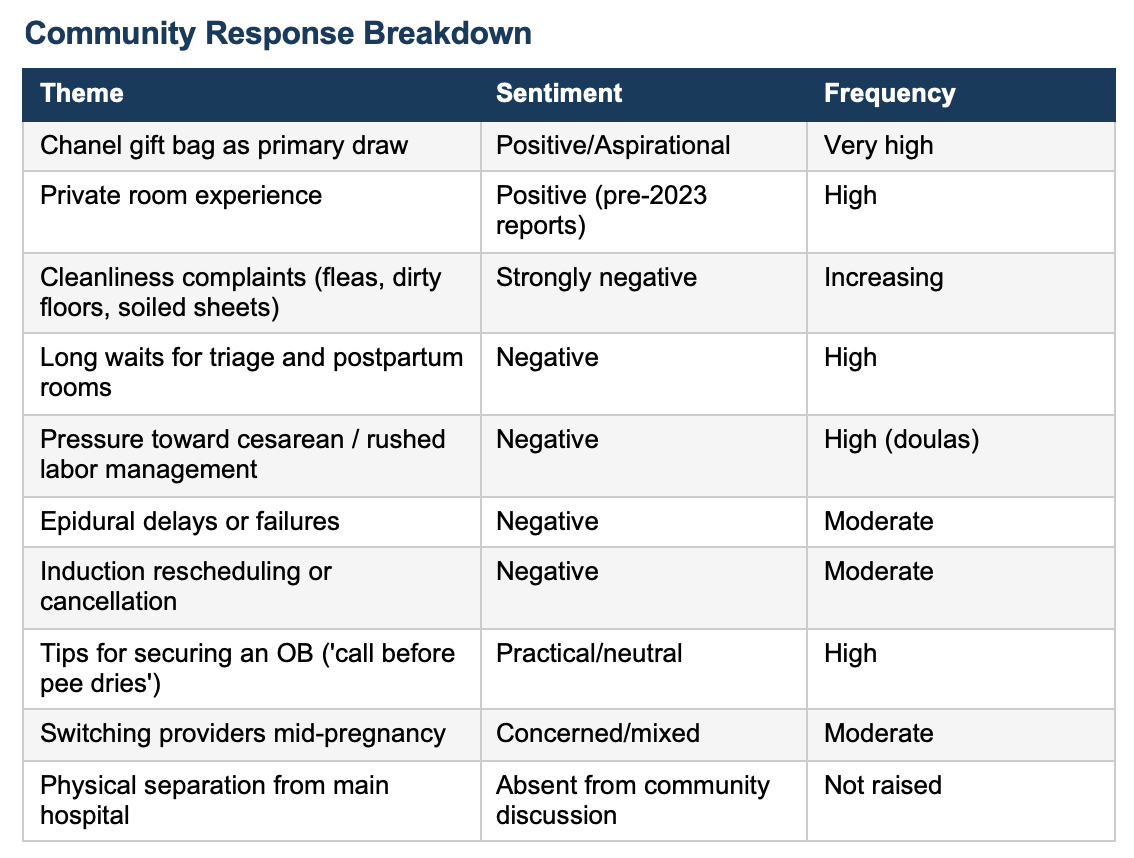
The only such unit in New York accepting high risk pregnant patients. Funded in part by a $75 million gift from hedge-fund billionaire Steve Cohen and his wife. It built its brand on private rooms, advanced technology, and Chanel gift bags for every patient. Online communities, Reddit, Facebook’s Moms of the Upper East Side, erupted with tips for securing admission, with patients describing calling their OB before the pregnancy test was dry.
According to the article in The Cut by 2024, those same communities were reporting flea bites traced to postpartum stays, sheets with holes, floors streaked with amniotic fluid, eight-hour waits for epidurals, and coordinated pressure to move patients toward cesarean delivery to free beds.
Ten doulas with hundreds of combined deliveries at the hospital described these problems as systemic. Not bad days, but a broken model.
Buried in the lifestyle reporting is a structural fact that no one in the community forums appears to have understood:
Alexandra Cohen is physically disconnected from the main hospital.
There is no tunnel.
There is no bridge.
A patient who deteriorates and cannot be taken care of there gets an ambulance if she needs a transfer.
We all have seen on TV emergency situations where patients are wheeled along a corridor to safety. That is not possible there because there is no corridor.
The emergency room is across the street.
Guess how many of the nearly 800-900 high risk Labor & Delivery units in the US have no physical hospital connection?
Do you want to be in the one that isn’t connected?
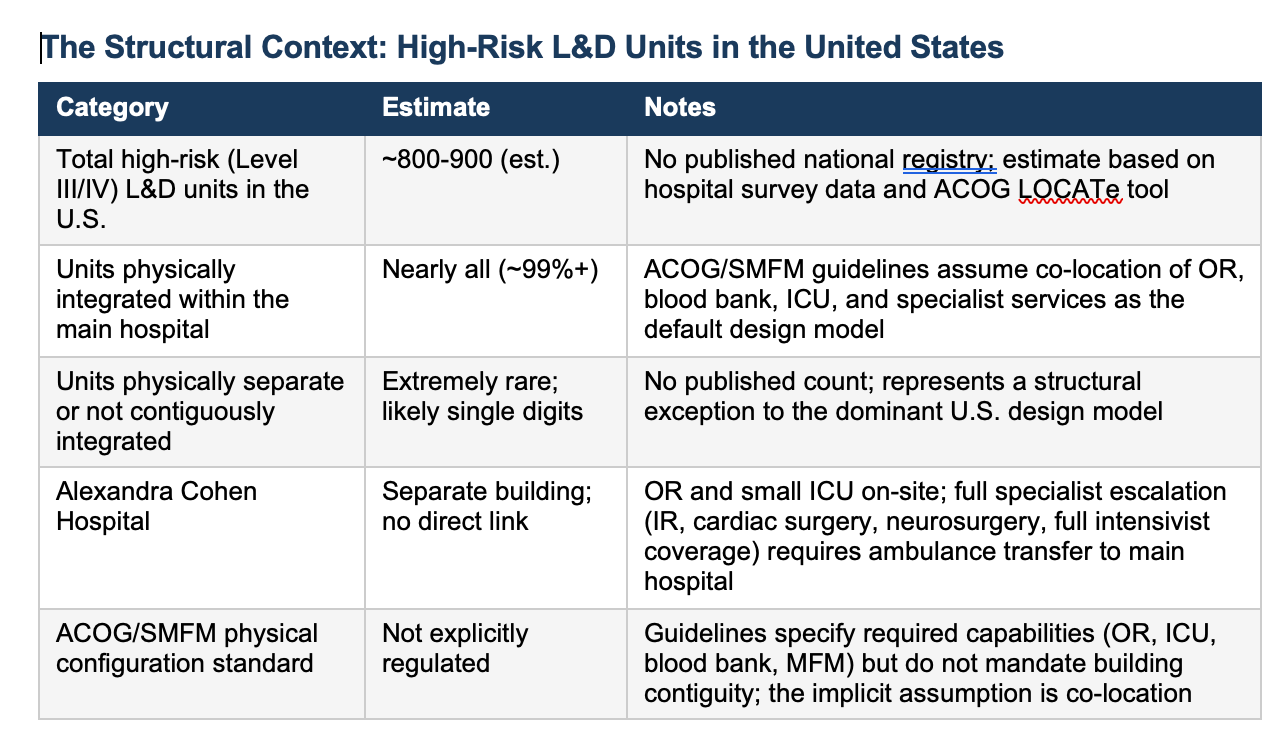
The ACOG/SMFM Levels of Maternal Care framework (Obstetric Care Consensus No. 9, 2019) defines Level III as subspecialty care and Level IV as regional perinatal health care centers -- the two tiers that handle high-risk obstetrics.
Both require an on-site OR, blood bank, MFM coverage, and an ICU that accepts pregnant and postpartum patients. The guidelines do not explicitly mandate that these resources share a building with the delivery unit. They do not need to.
Until Alexandra Cohen, the question had not arisen in any clinically meaningful way, because essentially all high-risk units in the United States are housed within their parent hospitals.
The guidelines assume co-location as the default. Alexandra Cohen is the exception -- and to our knowledge, the only one of its kind in New York City, and among a handful nationally.
The precise count of similarly configured units does not exist in any published registry, because the configuration is rare to the point that no one thought to count it.
Commentary
To be precise about what Alexandra Cohen has and what it does not have: the hospital has its own operating rooms. It has a small ICU. It has an on-site NICU. It has MFM coverage and anesthesia.
For the large majority of deliveries, even complicated ones, this is sufficient.
An emergency cesarean for nonreassuring fetal heart tones can be accomplished within the building. A postpartum hemorrhage that responds to uterotonics, uterine balloon tamponade, or surgical ligation can be managed on site.
For these scenarios, physical separation from the main hospital is a structural inconvenience, not a patient safety catastrophe.
The problem is not what Alexandra Cohen can handle. The problem is what happens when it cannot.
Obstetric emergencies do not announce their severity in advance. Uterine rupture, amniotic fluid embolism, placenta accreta spectrum discovered intraoperatively, peripartum cardiomyopathy, eclamptic intracranial hemorrhage, and refractory hemorrhage progressing to DIC are all conditions that can begin as apparently manageable situations and escalate within minutes to require resources that a self-contained six-floor unit does not possess.
The escalation pathway at Alexandra Cohen, for any condition exceeding what its own OR and small ICU can provide, is an ambulance.
Even for regular consults such as cardiac, pulmonary, dermatology, etc the specialists are across the street. Available, but delayed and inconvenient.
This is not an argument that Alexandra Cohen’s OR is inadequate, or that its ICU cannot stabilize a deteriorating patient. It can, and it does.
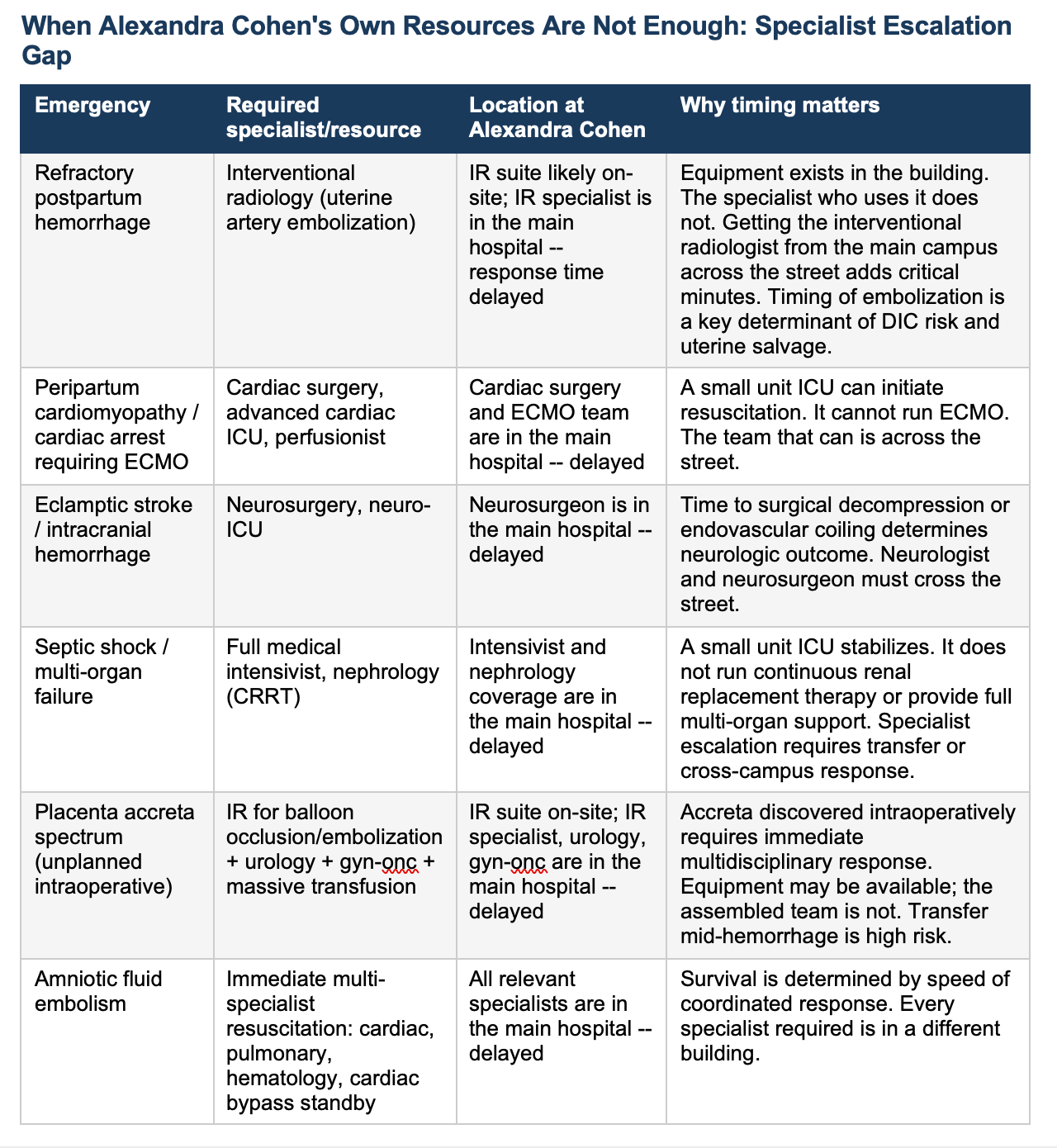
The argument is about specialist escalation: the interventional radiologist who must travel from the main campus to perform embolization in an IR suite that may sit in the building but goes unused without them, the cardiac surgeon and ECMO team for peripartum cardiomyopathy in extremis, the neurosurgeon for eclamptic intracranial hemorrhage, the full-capacity medical intensivist with continuous renal replacement therapy for multi-organ failure.
The equipment may be present. The specialists who operate it at the level these emergencies demand are not. They are across the street -- and in a city that does not stop for emergencies, across the street has a variable meaning depending on the time of day.
The literature on interventional radiology in obstetric hemorrhage is instructive here. Uterine artery embolization has become a standard second-line intervention for postpartum hemorrhage refractory to medical and surgical management, a fertility-preserving alternative to hysterectomy with well-documented efficacy. The evidence is also clear that timing matters: delay between hemorrhage onset and embolization increases the risk of disseminated intravascular coagulation and worsens outcome. Alexandra Cohen reportedly has an IR suite in the building. The suite is not the problem. The interventional radiologist is not in the building at all times. At a fully integrated Level III/IV center, the IR specialist is a phone call and an elevator ride away. Typically present in the hospital or on a short in-house call rotation. At Alexandra Cohen, that specialist is in the main NYP/Weill Cornell campus across the street, responding from wherever they are when the call comes in. In the middle of the night, with snow on the street. in the middle of a hemorrhage, the difference between an elevator ride and a street crossing is not trivial.
The IR suite being present means the procedure can happen once the specialist arrives. And his staff. It does not mean the specialist is there.
The volume argument compounds the structural one. The research literature on high-occupancy labor and delivery units is settled: higher census is independently associated with increased rates of emergency cesarean, instrumental delivery, and perineal laceration (Grobman et al., BJOG 2011; Snowden et al., BMJ 2015).
When ten experienced doulas (according to this article and comments) independently describe the same pattern, rushed inductions, patients held in triage to delay admission, Pitocin started and abandoned, cesarean offered as the solution to slow progres, they are describing a unit that has traded safety margin for throughput.
A unit operating at or near 7,000+ deliveries per year, in a building physically separated from full specialist support, has no margin for the unexpected. Every high-risk unit in the country operates on the assumption that the resources needed to rescue a deteriorating patient are steps, not streets, away.
The financial logic of this arrangement is not difficult to reconstruct. A dedicated women’s and newborns’ tower in a donor-funded building allowed NYP/Weill Cornell to brand a luxury product, capture market share, and generate lifetime patient revenue from a wealthy, privately insured population at scale. Obstetrics supposedly loses money on individual deliveries. Hospitals apparently claim they subsidize it because delivering 7,000 babies per year means 7,000 families who may bring their pediatric, gynecologic, cardiac, and oncologic care to the same system for decades. At that volume, in that zip code, the Alexandra Cohen model is not primarily a clinical project. It is a customer acquisition strategy with an OR attached. And the structural separation from full specialist support is the architectural consequence of building a luxury brand rather than a fully integrated tertiary care center.
None of this is hidden. The building is visible on the street. The ambulance protocol is, presumably, documented somewhere in the institution’s emergency transfer policies. What is not visible: to patients, to community forums, to the Reddit threads debating Chanel bag contents it is the implication:
That a hospital marketing itself to high-risk pregnancies, accepting complex MFM referrals, and operating the busiest L&D in New York City is doing so in a building where the full rescue infrastructure for its most catastrophic emergencies requires a street crossing.
What It Means
For patients choosing a birth hospital in New York City, the relevant questions should not be only about room aesthetics or gift bags.
They are: what is this hospital’s primary cesarean rate for first-time mothers? What are its nurse staffing ratios at peak census?
And -- the question no thread has asked -- if something goes wrong that exceeds what this building can manage, how long does it take to reach the specialist who can fix it?
At Alexandra Cohen, the honest answer to that last question is: we call 911. For a low-risk patient in uncomplicated labor, that may be an acceptable answer. For the high-risk patients this hospital actively recruits, prior cesareans, placenta previa, placenta accreta spectrum, complex cardiac disease, severe preeclampsia, it is a structural risk that has never been disclosed.
Women choosing Alexandra Cohen for high-risk care should be told, clearly and specifically, which emergencies can be managed in the building and which ones require an ambulance ride to the main hospital. That conversation is not happening.
New York State Department of Health publishes hospital-level cesarean rates and maternal outcome data. These are public records. They are more informative than any TikTok tour.
My Take
I have delivered over 10,000 babies. I have directed a major New York City labor and delivery unit. I have seen what it takes to run a safe floor at high volume, and I know the difference between a hard night and a broken system. In over 25 years in charge of a labor and delivery unit I have never had a maternal mortality on L&D.
I published about our safety program.
Let me be precise about what I am and am not saying about Alexandra Cohen’s physical configuration, because precision matters here.
I am not saying the hospital cannot perform an emergency cesarean. It can.
I am not saying its ICU cannot stabilize a critically ill postpartum patient. It can do that too. I am not saying that physical separation from the main hospital makes every delivery dangerous. For most patients, most of the time, it does not.
What I am saying is this: there is a category of obstetric emergency, unexpected, refractory hemorrhage requiring an interventional radiologist to run the embolization suite that sits in the building, peripartum cardiac collapse requiring a cardiac surgery team and ECMO, eclamptic stroke requiring a neurosurgeon, multi-organ failure exceeding a small ICU’s capacity, where the distance between where the patient is and where the specialist is becomes the determinant of survival. The equipment may be present. The people who operate it at the highest level of complexity may or may not be on site. At every other high-risk L&D unit in New York City, and at nearly every one in the United States, that specialist is measured in corridors and elevator rides away. At the prior L&D unit L&D was 3 floors and a dedicated elevator ride away from major help
At Alexandra Cohen, they are measured in city blocks and response times.
That is a structural fact. It is not disclosed in the marketing. It is not discussed in the community forums. It is not part of the informed consent conversation that high-risk patients have with their providers when choosing this hospital. It should be all three.
The Chanel bag was always a signal about what this institution was built to do.
It was built to attract wealthy patients, generate market share, and produce downstream revenue for a health system.
Those are legitimate business objectives. They are not the same as building the safest possible environment for high-risk obstetric care. When the two objectives conflict, as they potentially do every time a complex patient deteriorates beyond what six floors of a separate building can manage, the patient finds out which one was the priority.
The women who chose this hospital deserve to know that before they needed to find out.
That is what an informed consent is all about.
I worked at a hospital in SW Michigan, the only facility in a 9 county radius that had MFM providers - L&D was in a different building 1/4 mile away from the main hospital. Lost a mom of triplets due to hemorrhage and not getting enough blood quickly enough. That was one case, there were others.
Women’s health is still marginalized at every level in every community.