
Is This Why Mothers Die More Often in the United States Than in Europe?
The structural differences in insurance, prenatal care, and hospital organization that shape obstetric outcomes.

The United States and Germany both practice advanced medicine. Yet the organization of care, the role of physicians, and the structure of prenatal services reveal two very different medical cultures.
At first glance, medicine in the United States and Germany looks remarkably similar. Both countries train highly skilled physicians, rely on modern hospitals, and practice evidence-based medicine. Yet beneath that shared scientific foundation lies a system shaped by very different structures, professional roles, and expectations about how care should be delivered.
Even the language of medicine reflects the difference. In the United States physicians in training are residents, supervised by attendings.
In Germany they are Assistenzärzte, supervised by Fachärzte or Oberärzte, with department leaders called Chefärzte.
American hospitals speak of labor and delivery units, emergency departments, and attendings.
German hospitals refer to Kreißsäle, Notaufnahmen, and Dienstärzte. The terminology signals different professional hierarchies and different traditions in how authority is structured within hospitals.
Prenatal care also begins in different places.
In Germany most pregnant women receive routine prenatal care from community-based office obstetricians or gynecologists (Frauenärzte). These physicians typically operate in private outpatient practices and follow standardized national prenatal care schedules. Insurance coverage is nearly universal through statutory health insurance or private insurance, so access to prenatal visits, ultrasounds, and laboratory testing is rarely limited by coverage status.
All patients in Germany can see a doctor in her practice
In the United States the situation is more fragmented. Prenatal care depends heavily on insurance status. Some pregnant women receive care through private insurance plans with broad access to specialists and imaging. Others rely on Medicaid, which finances a large share of births but varies by state in provider participation and reimbursement.
There is rarely a private physician in the US seeing a Medicaid patient in her practice
A smaller group of women begins pregnancy without insurance and may delay care until Medicaid eligibility is established or until they reach hospital systems that provide safety-net services.
Insurance also influences where women give birth in the United States.
Some hospitals predominantly serve privately insured patients, while others function as safety-net institutions caring for large Medicaid or uninsured populations. As a result, the distribution of obstetric patients across hospitals often mirrors the structure of the insurance system itself.
Germany operates differently.
Nearly all residents are insured through a universal system of statutory health insurance funds. Hospitals generally care for patients regardless of insurance fund membership, and pregnant women are usually directed to hospitals based on geography, physician referral, or patient preference rather than insurance status.
Hospital labor care reflects additional differences. In Germany, as in much of Europe, midwives play a central role in labor management. Physicians are present for complications, operative deliveries, and surgical care, but routine labor is frequently managed by midwives. German hospitals also commonly provide extended postpartum inpatient stays, historically several days after delivery.
In the United States obstetric care is typically organized around physician-led teams supported by labor nurses, anesthesiologists, and neonatal specialists. Postpartum stays tend to be shorter, and hospital throughput pressures are greater.
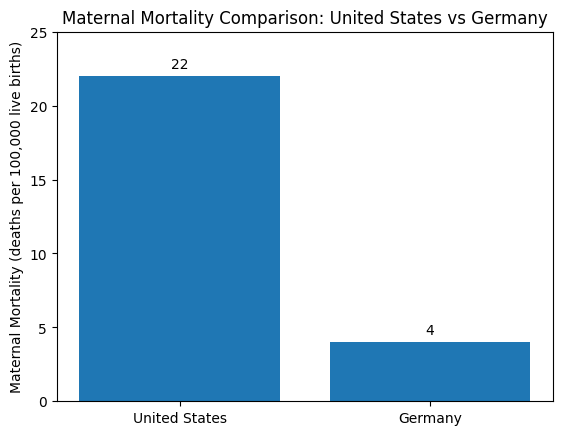
These structural differences occur alongside differences in national outcomes. Maternal mortality is substantially higher in the United States than in Germany. Recent national statistics report maternal mortality ratios in the United States of roughly 20 to 30 deaths per 100,000 live births, depending on the year and methodology, while Germany reports approximately 3 to 7 deaths per 100,000 births. Neonatal mortality is also somewhat higher in the United States, although the difference is smaller.
Interpreting these differences is complex. Maternal mortality reflects not only hospital care but also population health factors such as chronic disease, obesity, maternal age, access to prenatal care, and social determinants of health. Differences in how deaths are reported and classified may also influence comparisons between countries.
Both systems therefore show strengths and tensions.
Germany offers near universal coverage, strong outpatient prenatal care networks, and relatively consistent access to maternity services.
The United States offers rapid access to advanced subspecialty care and technological innovation, but access to routine prenatal services can vary depending on insurance coverage and regional resources.
The deeper difference is philosophical. German medicine developed within a regulated insurance framework designed to guarantee coverage for the entire population. American medicine evolved through a complex mix of private insurance, employer-based coverage, public programs such as Medicaid and Medicare, and hospital-based care systems.
These historical choices still shape clinical practice today.
Spend time in a German maternity clinic and then walk through an American labor unit. The science of obstetrics is the same. The textbooks are the same.
But the organization of care feels different. And outcomes are very different. More than fives times more women die in the US in and after pregnancy.
Sometimes profoundly so.