

The CDC definition of maternal death excludes homicide, suicide, and drug overdose. A new NEJM paper shows those three causes account for more than one in four pregnancy-associated deaths. We are not counting the bodies correctly -- and that has consequences.
Here is the official definition of a maternal death, straight from the CDC, borrowed word for word from the World Health Organization:
“The death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.”
Read it again. Slowly. “Not from accidental or incidental causes.”
Who decides what is accidental?
Who decides what is incidental?
The definition does not say.
A coroner decides.
A death certificate coder decides.
A bureaucrat with an ICD-10 lookup table decides. And because of that quiet, unremarkable decision, homicide does not count as a maternal death. Suicide does not count. A fatal drug overdose does not count.
We call our maternal mortality statistics a public health crisis. We are not even counting the right deaths.
What the data actually show
A study published in the New England Journal of Medicine in February 2026 analyzed all maternal deaths in the United States from 2018 through 2023 -- 7,901 deaths total. The leading cause of death was not hemorrhage, not preeclampsia, not sepsis. It was unintentional drug overdose: 1,152 deaths, or 5.2 per 100,000 live births. The second leading cause was violence -- defined as homicide or suicide -- with 866 deaths: 3.9 per 100,000 live births. Together, overdose and violence killed more pregnant and postpartum women than cardiovascular disease, infection, hypertension, and hemorrhage combined.
And none of those deaths appear in the official maternal mortality rate. By definition, they cannot. They are “accidental or incidental.”
A larger analysis presented at the Society for Maternal-Fetal Medicine’s 2025 annual meeting examined CDC data from 2005 to 2022 -- 20,421 maternal deaths.
Of those, 2,293 (11 percent) were from homicide or suicide. Sixty-one percent were homicides. Thirty-nine percent were suicides. Fifty-five percent of violent deaths involved a firearm.
Black women aged 18 to 24 died from homicide at nearly four times the national average.
These are not incidental deaths. They are not coincidental deaths. They are deaths that happen because a woman is pregnant or has recently given birth -- and the official definition will not count them.
The logical problem at the center of the definition
Let us think about suicide first. A woman develops postpartum depression -- a recognized, direct complication of childbirth. Her depression goes untreated or undertreated. She dies by suicide six weeks after delivery. Under the current definition, this death is accidental or incidental. The pregnancy that triggered her depression does not make the list.
Now consider homicide. Research has documented for decades that pregnancy increases a woman’s risk of being killed by an intimate partner. The risk does not stay constant -- it rises with the pregnancy. Announcing a pregnancy to the wrong person has ended lives. Being pregnant and unable to leave has ended lives. In more than half of pregnancy-associated homicides in one multi-state study, the obstetric provider already knew about or suspected intimate partner violence. The pregnancy was not incidental to the murder. The pregnancy was the context in which the murder happened.
The lead author of the SMFM study said it plainly:
“Being pregnant or postpartum significantly increases the risk of death by homicide, and more pregnant women die of violence than any individual medical cause. Part of the reason violence is not recognized as the leading cause of death during pregnancy is because we don’t include homicide and suicide in the definition of maternal mortality.”
That is not a minor technical quibble. That is a definition actively hiding the leading causes of death in pregnant women.
What this means for patients
If you are pregnant or recently gave birth, the biggest risks to your life are not what most people think. Bleeding and infection are serious. Preeclampsia is serious. But statistically, violence and drug overdose kill more pregnant women in this country than any single obstetric complication.
Because these deaths are not included in official maternal mortality statistics, there is less urgency to fund screening programs, less urgency to train providers to ask the right questions, and less urgency to treat intimate partner violence as a clinical emergency. What does not get counted does not get funded. What does not get funded does not get fixed.
The pregnancy checkbox on the death certificate has been a source of persistent misclassification problems for years. The CDC itself acknowledges that erroneous entries create overcounts, especially in women over 40. We spend effort correcting those errors. We spend far less effort asking whether the entire definitional framework is wrong.
My take
I have been working with the CDC natality database for many years. I understand why the WHO definition exists and why the CDC adopted it -- it provides international comparability, it focuses attention on obstetric causes that are preventable through clinical intervention, and it avoids counting car accidents that happen to involve pregnant women. I understand the logic.
I do not accept the result.
A definition that excludes the leading cause of death in the population it is supposed to measure is not a conservative definition. It is a wrong definition. The word “incidental” does real harm when it is applied to a postpartum suicide or a homicide by an intimate partner. These are not incidental events. They are deaths causally connected to pregnancy -- through the physiology of postpartum mood disorders, through the social vulnerability of pregnancy, through the control dynamics that intimate partner violence exploits.
The definition needs to be revised. It should distinguish between a death that is truly incidental to pregnancy -- a car accident with no obstetric connection -- and a death that is causally linked to the pregnant or postpartum state, even if the mechanism of death was violence. The tools exist to make that distinction. The will to make it has been missing.
We keep asking why the United States has the worst maternal mortality rate in the developed world. Part of the answer is that we are not measuring it correctly. The true number is worse than what we report. And we built the reporting system that way.
ObGyn Intelligence covers what the data actually show, not what the definition allows us to see. If that is the kind of evidence-based analysis you want, subscribe below.
References
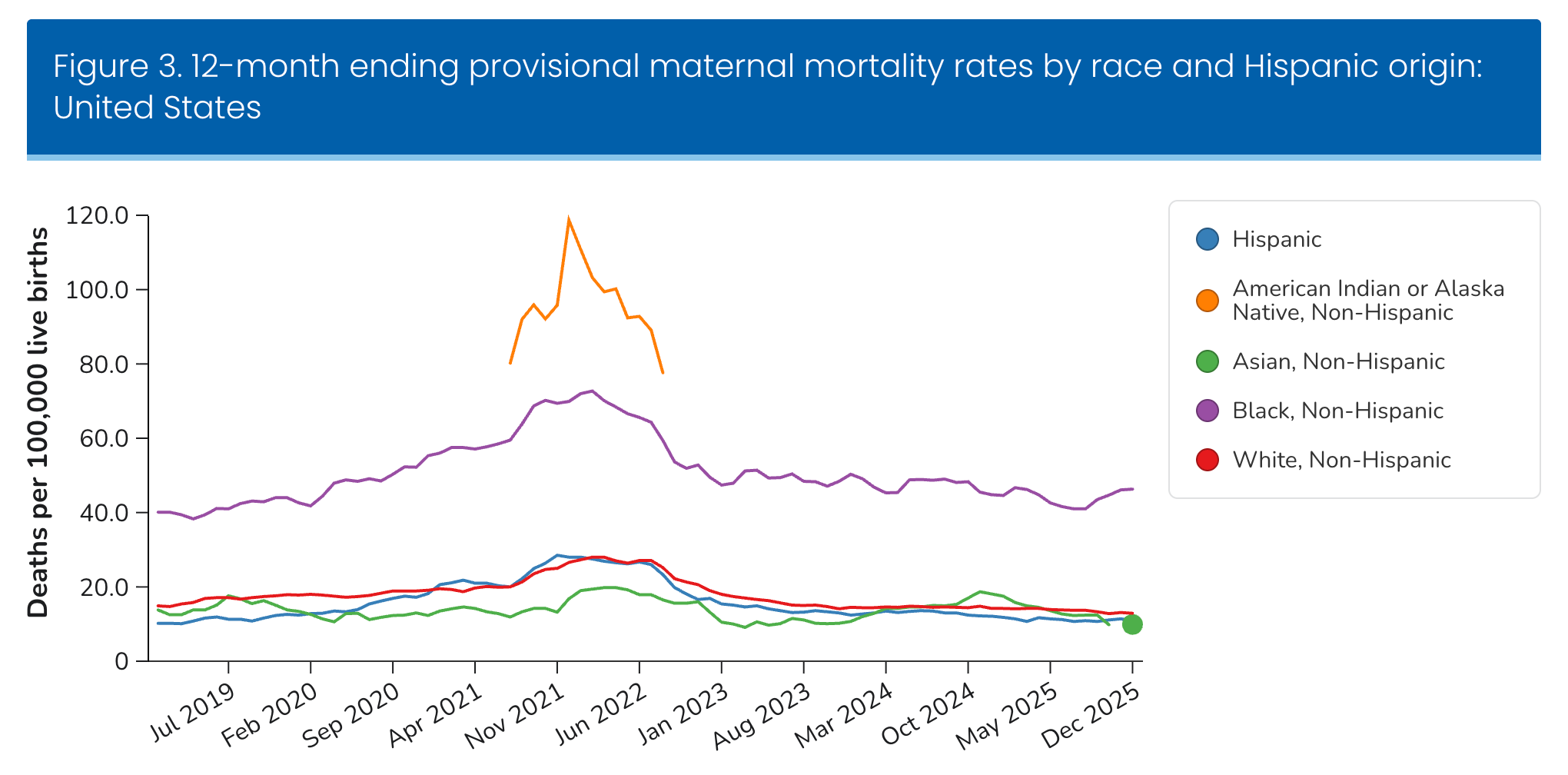
1. National Center for Health Statistics. Provisional Maternal Death Rates. Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/nchs/nvss/vsrr/provisional-maternal-deaths-rates.htm
2. Azad HA, et al. Overdose, Homicide, and Suicide as Causes of Maternal Death in the United States. N Engl J Med. 2026 Feb.
3. Azad HA, et al. Homicide and Suicide as Leading Causes of Maternal Death in the United States. Presented at SMFM The Pregnancy Meeting 2025.
4. Wallace ME, Hoyert D, Williams C, Mendola P. Pregnancy-associated homicide and suicide in 37 US states with enhanced pregnancy surveillance. Am J Obstet Gynecol. 2016;215(3):364.e1-364.e10.
5. Palladino CL, Singh V, Campbell J, Flynn H, Gold KJ. Homicide and suicide during the perinatal period: findings from the National Violent Death Reporting System. Obstet Gynecol. 2011;118(5):1056-63.
6. National Center for Health Statistics. Vital Statistics Reporting Guidance No. 4: A Reference Guide for Certification of Deaths Associated With Pregnancy on Death Certificates. CDC; 2022.