
She Trusted Her Body. The Monitor Proved Her Right.
What 77 Comments About Decreased Fetal Movement Reveal About a Critical Safety Gap


What Is Decreased Fetal Movement?
Decreased fetal movement (DFM) means a pregnant woman notices her baby moving less than usual. It is one of the most important warning signs in the third trimester. Fetal movement reflects fetal wellbeing. A baby that is stressed, compromised by placental dysfunction, or suffering from reduced oxygen delivery will often reduce its movement to conserve energy. This is the biology behind why DFM matters.
DFM does not mean the mother imagined it. It does not mean she is overreacting. It does not go away by drinking cold water or lying on her left side. Those interventions are outdated and, more importantly, they delay evaluation. The UK’s NICE guideline explicitly advises women not to try to stimulate movement at home but to contact their care provider immediately. The reason is straightforward: if a baby needs stimulation to move, that is a clinical finding, not a reassurance.
Normal fetal movement varies widely between pregnancies and changes with gestational age. What matters is a change from the individual baby’s established pattern. A woman who knows her baby moves constantly and suddenly notices hours of silence is reporting a clinical symptom, not anxiety. The conditions associated with DFM include placental dysfunction, oligohydramnios (low amniotic fluid), umbilical cord complications, and in severe cases intrauterine fetal demise. Evaluation requires electronic fetal monitoring and, when indicated, ultrasound assessment of fluid and biophysical profile.
The standard of care, supported by evidence and endorsed by ACOG and NICE alike, is this: when a pregnant woman reports decreased fetal movement, she should be evaluated. Not reassured over the phone. Not told to try juice and wait. Evaluated.
Summary
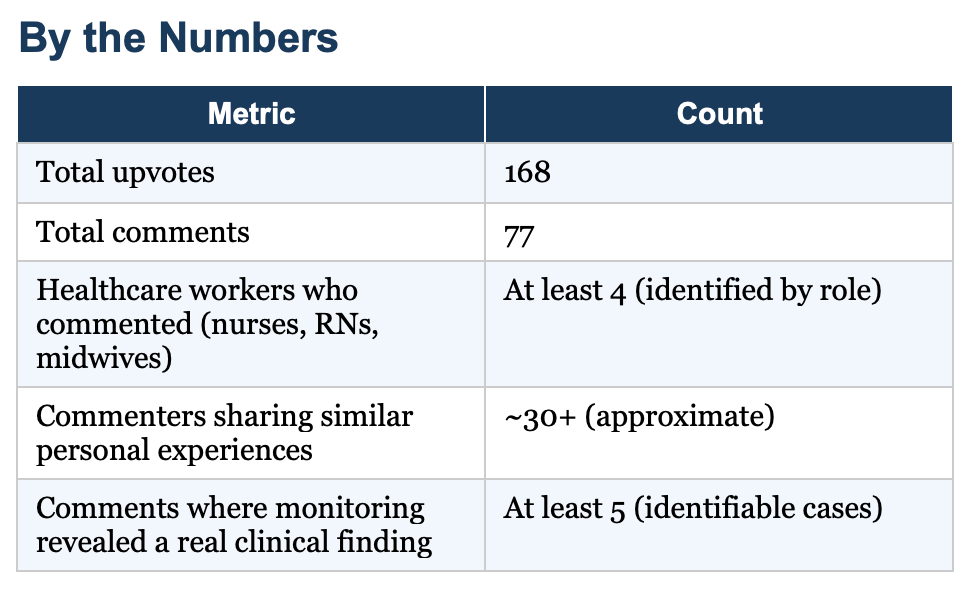
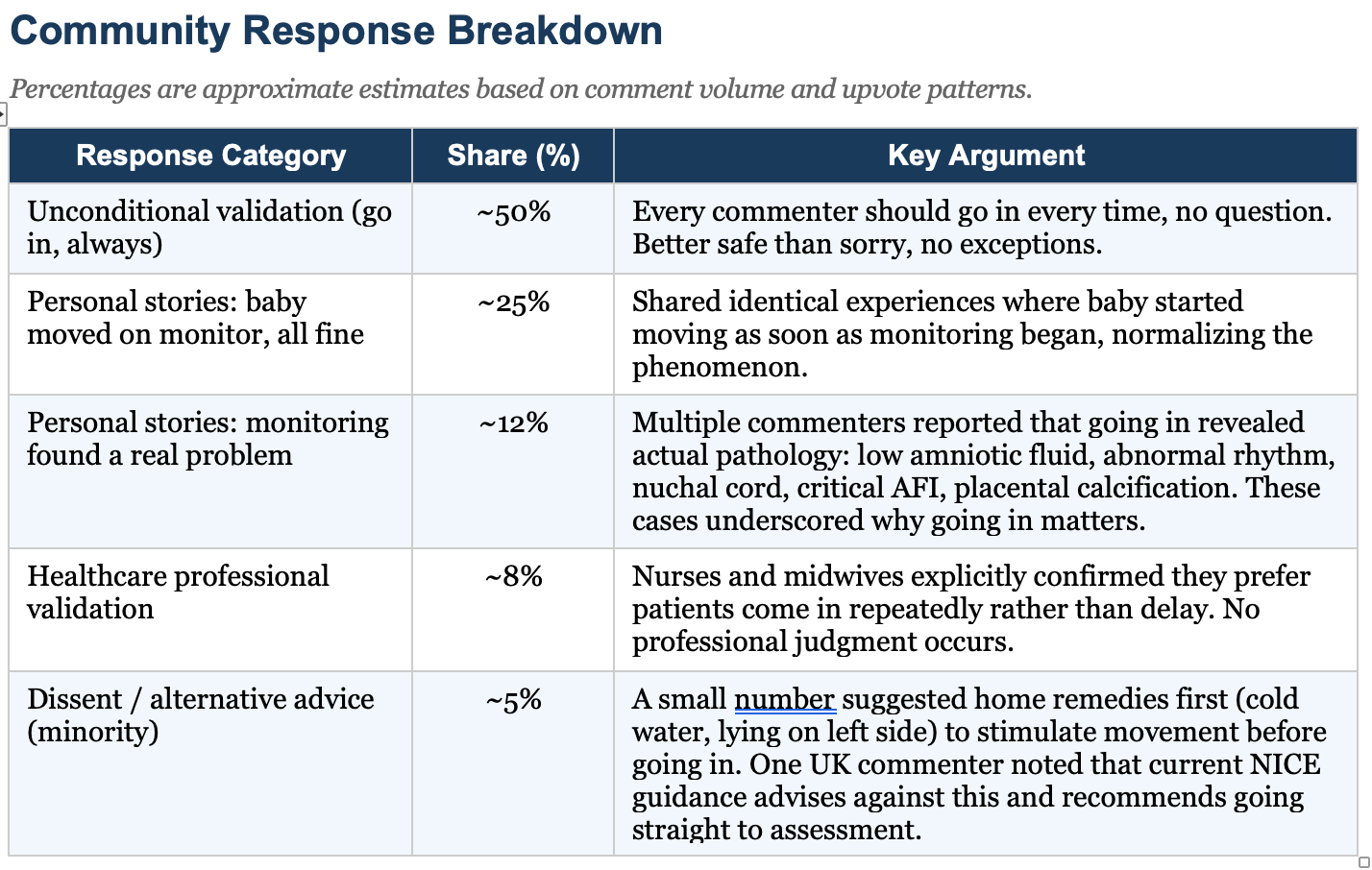
A woman at 28 weeks and 4 days posted to r/pregnant after spending several hours not feeling her baby move. She went to the hospital, where monitoring showed active fetal movement she could not perceive. She felt embarrassed. The post received 168 upvotes and 77 comments. The comment section became a sustained, community-led affirmation that she did the right thing. Multiple commenters shared identical experiences. Several shared experiences where going in led to the discovery of a real clinical problem. Healthcare workers in the thread confirmed without exception that evaluation is always appropriate for decreased fetal movement.
What It Means
The thread documents something clinically important: women are still being made to feel that reporting decreased fetal movement is excessive. This woman was not comforted by her clinical experience. She was embarrassed by it. That embarrassment is a patient safety problem. A woman who feels dumb for going in once is less likely to go in again. That hesitation is where babies are lost.
Do the fetal kick count HERE.
The cases buried in the comments illustrate the clinical reality. One woman reported low amniotic fluid leading to induction. Another described a baby with a critical AFI and placental calcification discovered only because she went in. A third woman needed an emergency cesarean for fetal distress, identified on her second visit in one week, after she almost did not call because she felt she had already been in too recently. In each case, the presenting symptom was what this original poster experienced: a decrease from a known movement baseline.
The fact that monitoring revealed movement the mother could not feel is not a false alarm. It is a reminder that maternal perception of fetal movement is an imprecise but meaningful clinical tool. Anterior placenta position, fetal position, gestational age, and amniotic fluid volume all affect what a mother can perceive. The monitors pick up what maternal touch cannot. That is the point of going in.
My Take
This thread reveals a gap that no guideline has closed: the space between what evidence says and how women feel when they act on it. Every professional organization that has addressed decreased fetal movement recommends prompt evaluation.
The evidence for maternal perception as an early warning system is not in dispute.
Yet a 28-week patient with a history of an active baby went to the hospital after hours of silence and came home embarrassed.
That is a failure of clinical communication, not of clinical care. The nurses were apparently kind. The evaluation was appropriate. But nothing in her encounter neutralized the social signal she had received somewhere, from someone, that going in for this concern was excessive. The thread normalized her experience in a way her clinical encounter did not.
One comment, from a woman who nearly stayed home because she thought she was imagining things, stood out. She went in. Her AFI was critically low. She was monitored for three weeks and induced at 36 weeks. The placenta had begun calcifying. She wrote: ‘Without the monitoring we wouldn’t have known until it was too late.’ That is the case for going in. Every time.
The clinical message should be framed not as ‘come in if you’re worried’ but as ‘a change in your baby’s movement pattern is a symptom, and symptoms deserve evaluation.’ Worry is subjective. A symptom is a clinical fact. We do not tell patients with chest pain to try lying down first to see if it goes away. We should stop implying that to pregnant women reporting decreased fetal movement.