
“The Case for Cash-Based Care -- Physicians Debate Whether Opting Out Is Ethical” ObI | The Digital Waiting Room

Doximity is where doctors go at 2 a.m.
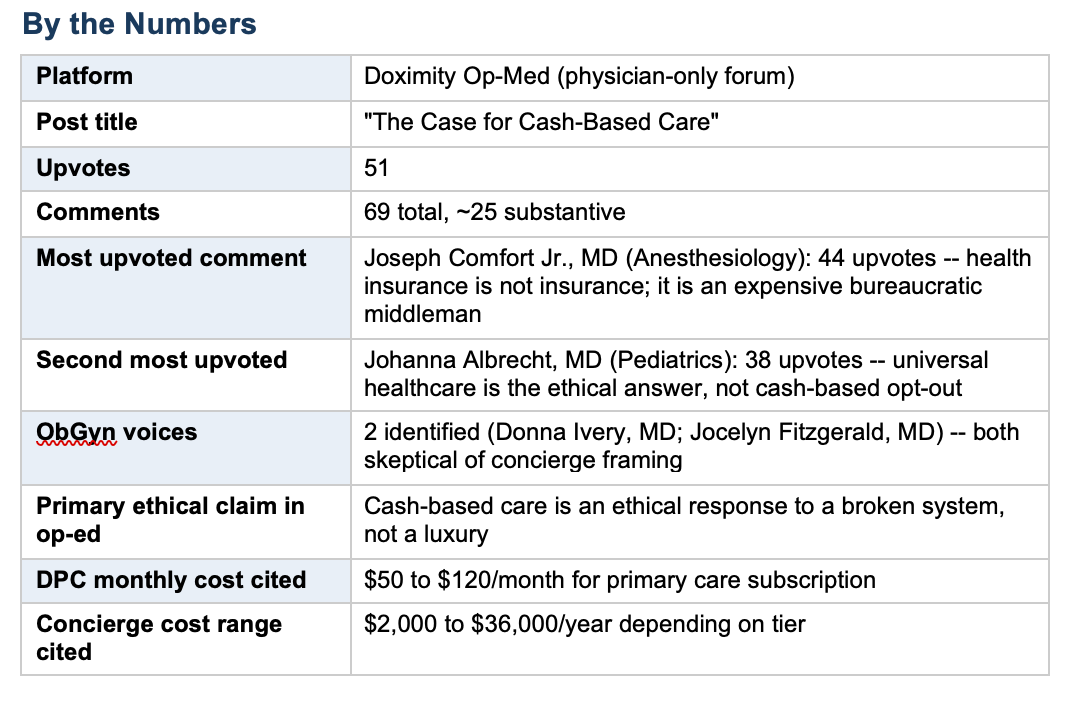
This week’s thread comes from Doximity’s Op-Med forum, a physician-only platform where, it turns out, doctors can be just as unfiltered as anonymous internet users, only with credentials.
An Op-Med essay arguing that cash-based care is an ethical response to a broken system drew 69 comments and 51 upvotes from physicians across specialties. The arguments ran the full spectrum: libertarian (no one has a right to another’s labor), structural (insurance is the real villain), practical (DPC works for routine care, not for catastrophes), and moral (concierge medicine serves the privileged, abandons the rest).
Missing almost entirely: any acknowledgment that physicians carry a professional obligation that distinguishes us from plumbers, hair stylists, and tax accountants: the comparison several commenters volunteered without apparent irony.
The thread is a useful artifact of how physicians rationalize individual exit strategies as ethical acts while the system they are exiting continues to fail the patients who cannot follow them out the door.
Evidence-Based Commentary
Let us start with the ethical sleight of hand at the center of this entire debate.
The Op-Med essay frames cash-based care as an ethical response to a broken system. That is a grammatically coherent sentence that collapses under the slightest pressure. An ethical response to a broken system is one that works to fix it, advocates for patients within it, or at minimum does not make it harder to fix by removing the physicians most capable of demanding change. Opting out and calling it ethics is not a response -- it is a resignation letter dressed up as a manifesto.
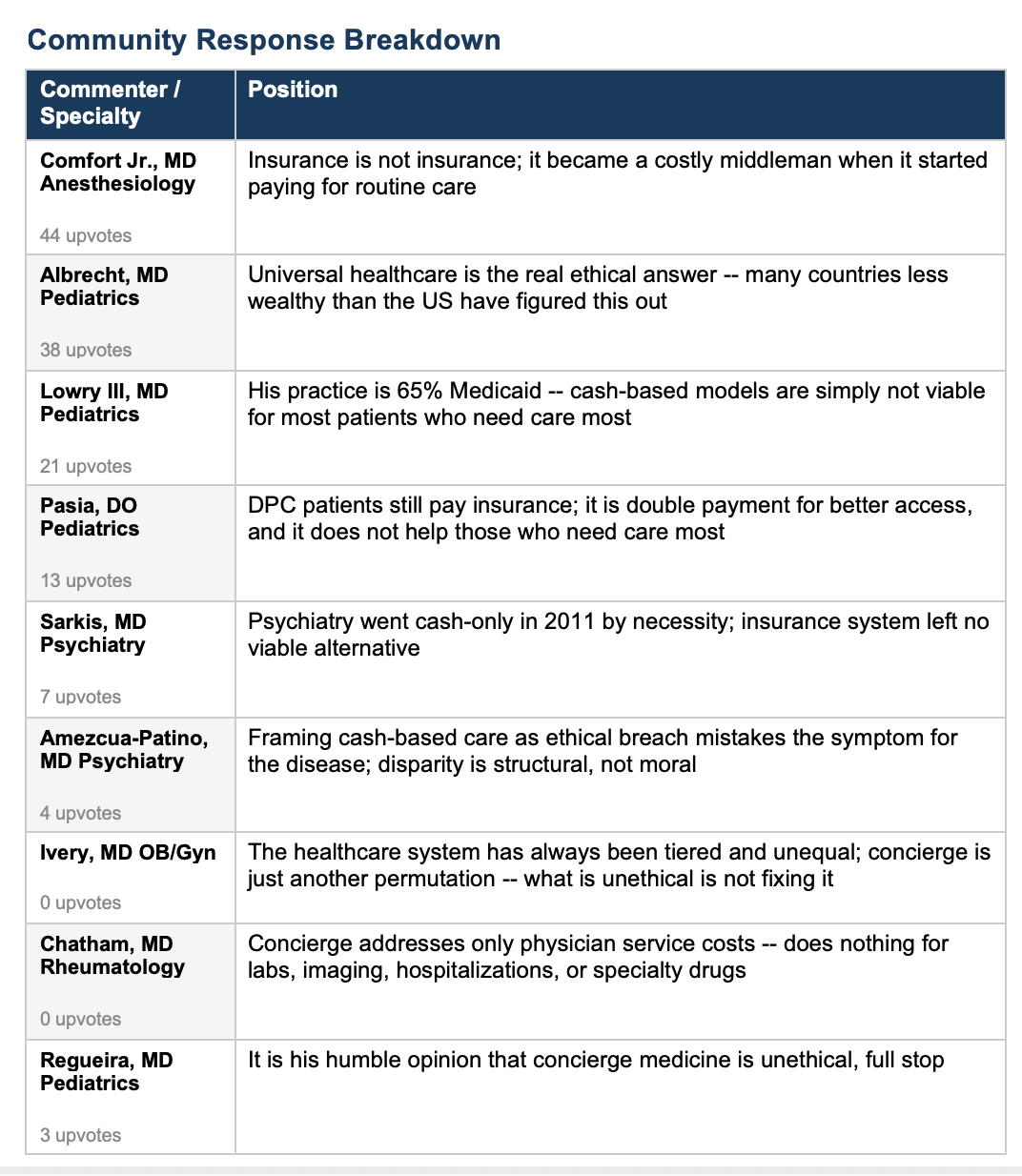
The most upvoted comment in the thread (44 upvotes) argues that health insurance stopped being real insurance when it began covering routine care, comparing it to auto insurance that does not pay for oil changes. This analogy is rhetorically satisfying and analytically useless. An oil change does not prevent your car from catastrophically failing and killing other people on the highway. Untreated hypertension, gestational diabetes, and cervical dysplasia are not oil changes. The entire moral architecture of medicine -- from the Hippocratic tradition to modern bioethics -- is built on the premise that medical care is not a commercial transaction like any other, precisely because the stakes are different and the information asymmetry between physician and patient is profound.
Several commenters invoked the plumber comparison. A plumber charges what the market will bear; why should a physician be different? Because a plumber has not taken an oath. Because a plumber is not granted a legal monopoly on a service that people cannot survive without. Because medical licensing exists as a social contract: society grants physicians extraordinary privilege -- prescription authority, hospital access, legal protections -- and in exchange, physicians accept professional obligations that ordinary tradespeople do not carry. The moment you cash that check, you have agreed to the terms. You do not get to redesign the contract when it becomes inconvenient.
The professional responsibility framework, which I have applied in my work for decades, is unambiguous on this point. Professional responsibility is not a preference. It is not a lifestyle choice contingent on favorable reimbursement rates. It is the foundational ethical obligation that justifies the profession’s existence and its social privileges. When physicians frame individual practice decisions as ethical acts without accounting for their population-level consequences, they are not doing ethics, they are doing rationalization.
The structural critique buried in this thread is legitimate and largely correct: insurance as currently constituted is extractive, bureaucratic, and organized primarily around the financial interests of intermediaries rather than patients. This is empirically true. It does not follow, however, that the ethical corrective is for individual physicians to exit the system and serve a smaller, wealthier panel. That is precisely analogous to arguing that because public schools are underfunded, private school tuition is an ethical act. It describes a personal solution. It does not constitute a remedy.
The only ObGyn voices in this thread -- Donna Ivery and Jocelyn Fitzgerald -- both point in the right direction. Dr. Ivery notes that the American healthcare system has always been tiered and inequitable, and that concierge medicine is simply another iteration of a structure that has never served everyone. Dr. Fitzgerald’s brief contribution -- ‘This is what is happening in endometriosis care’ -- says everything. Endometriosis takes an average of seven to ten years to diagnose. That delay is not shortened by cash-pay practices for patients who can afford them. It is shortened by structural accountability, better training, and a healthcare system that takes women’s pain seriously regardless of income. The cash-based model addresses none of that.
One comment from a rheumatologist deserves particular attention for its precision: concierge practice may improve physician service delivery for patients without Medicaid, but it does nothing to address the largest patient costs, laboratory studies, imaging, emergency department visits, hospitalizations, or specialty medications. This is correct.
The entire cash-based care argument addresses the least expensive component of a patient’s healthcare expenditure and leaves the catastrophic costs entirely untouched. A patient in a DPC practice who develops ovarian cancer, a pulmonary embolism, or preeclampsia is not protected by her monthly subscription fee. She is on her own with whatever insurance she could afford -- which in a DPC model, the physician conveniently will not be managing.
Finally, the ethics framing itself demands scrutiny. The original essay argues that in a broken system, cash-based care may be an ethical response. May be. The epistemically humble hedge of a conclusion that cannot survive direct examination. Real ethical analysis requires asking not only whether an action is permissible for the individual, but what the consequences are for those who cannot make the same choice. In bioethics, we call this the justice principle. It is not optional. A practice model that improves care for patients who could already navigate the system adequately, while accelerating the deterioration of care for patients who cannot, fails the justice analysis regardless of how liberating it feels for the physician choosing it.
What It Means
The cash-based care debate is a symptom of genuine physician burnout, administrative burden, and a reimbursement system that undervalues primary and preventive care. These are real problems. The ethical response to real problems, however, is not to reframe personal accommodation as moral courage. When physicians argue that opting out is ethical because the system is broken, they are making a claim that requires them to account for who gets left behind when they leave. That accounting is notably absent from this thread and from most cash-based care advocacy. Professional ethics in medicine is not satisfied by improving your own working conditions. It requires attending to the obligations that exist precisely because physicians hold a privileged position in society -- obligations that persist even when, especially when, the system makes honoring them inconvenient.
My Take
I have been inside this system for more than 50 years. I have delivered over 10,000 babies, directed a large Labor and Delivery unit, fought with insurers, navigated administrative nightmares, and watched colleagues burn out in real time.
I understand the appeal of opting out. I understand it viscerally.
But I cannot call it ethics. Nor should you.
The physicians in this thread who invoke libertarian philosophy, no one has a right to another’s labor, are technically correct and professionally irrelevant.
Of course no one has a claim on your labor in the abstract. But you chose medicine. You accepted the license, the privileges, the title, and the social trust that comes with it. That trust was built by generations of physicians who did not opt out when things got hard.
Calling your exit strategy an ethical act does not make it one. It makes it a rationalization, and a well-upvoted one, at that.
The obstetricians in this thread mostly said the right things. The rest of medicine has more work to do.