

Paul Krugman published an essay this week about private credit and financial risk. He was writing about money. But I kept reading it as if it were about obstetrics.
His central argument is this: financial crises do not happen because one thing goes wrong. They happen because deregulation, institutional amnesia, opacity, and tolerance of systemic risk all accumulate quietly until the pressure exceeds what the system can hold. The cockroaches, as Jamie Dimon put it, are there long before anyone turns on the light.
Replace “private credit” with “American obstetrics” and the essay reads as a near-perfect description of the maternal and neonatal mortality crisis in the United States.
The Numbers That Should Not Exist
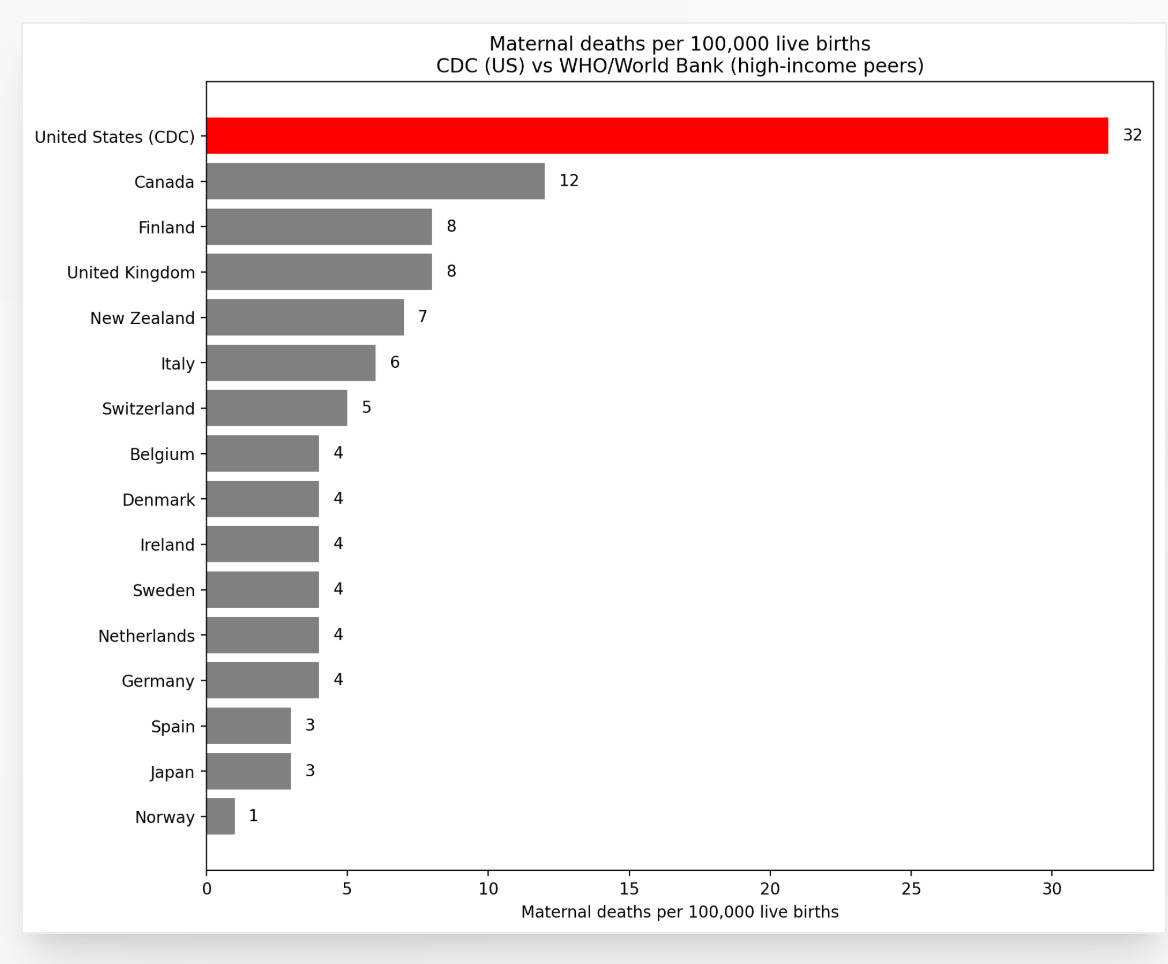
The United States has the highest maternal mortality rate among high-income countries. Not slightly higher. Dramatically higher. In 2022, the CDC reported a maternal mortality ratio of 22.3 deaths per 100,000 live births. The comparable figures for Germany, France, and the United Kingdom were between 4 and 9. We are not talking about a gap that requires a microscope. We are talking about a gap that requires an explanation.
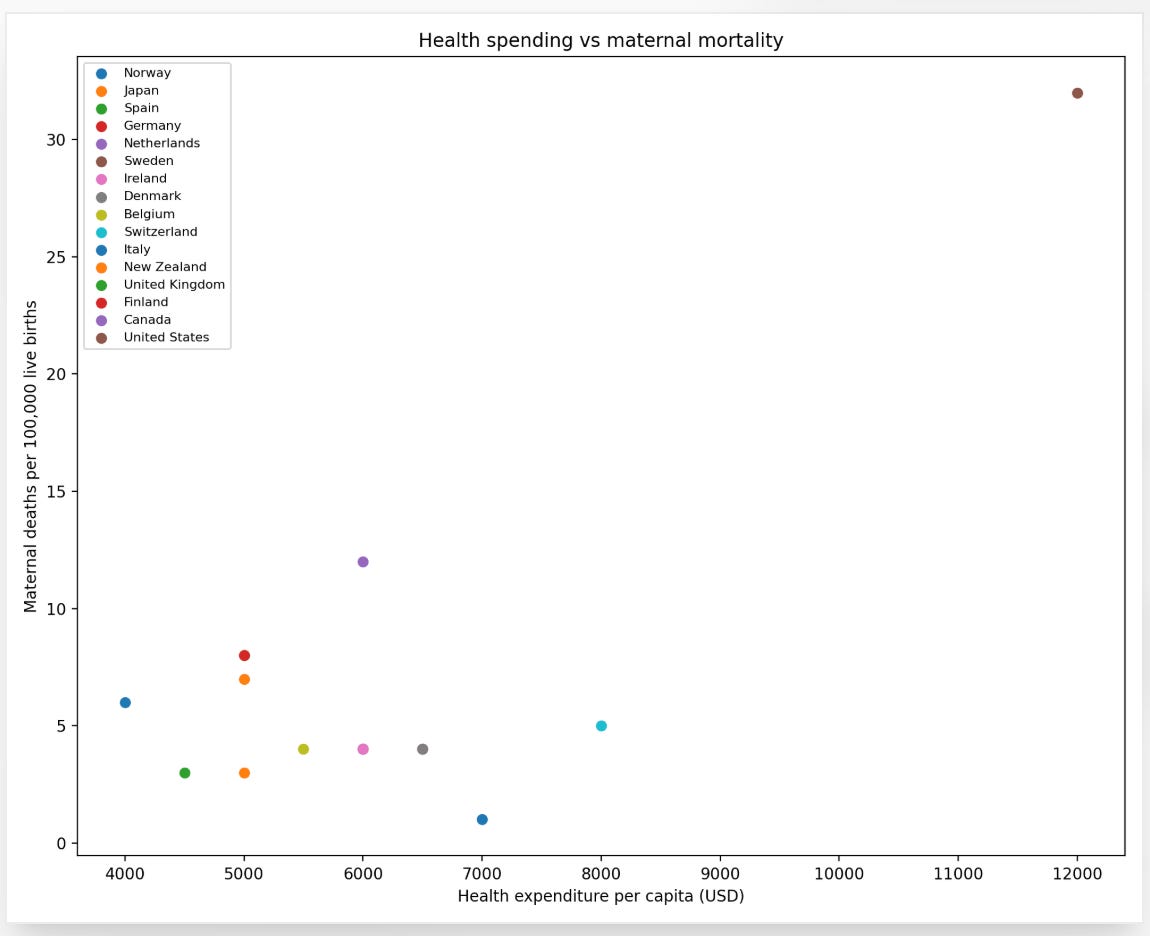
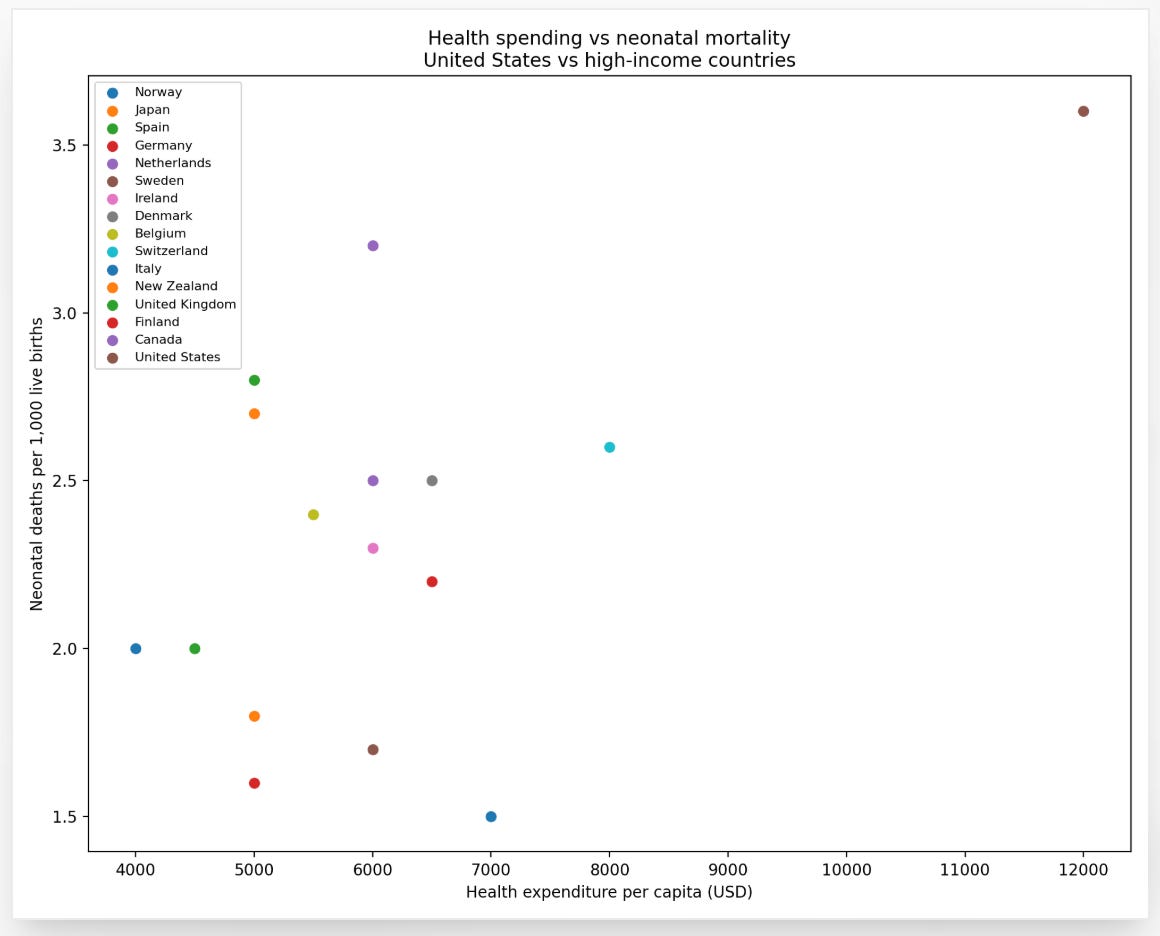
Neonatal mortality tells a similar story. For a country that spends more per capita on healthcare than any other nation on earth, the outcomes are not merely disappointing. They are a scandal.
How is this possible? The same way Krugman’s financial crises happen. Not one catastrophic failure. A slow accumulation of smaller ones, each normalized, each explained away, each generating its own institutional defense.
Deregulation: The Quiet Period Is Over
Krugman describes a “quiet period” in American finance, roughly 50 years after the 1930s, when regulators mostly won the arms race against risk-taking. American obstetrics had its own quiet period, roughly the middle decades of the twentieth century, when hospital birth became universal, neonatal intensive care units arrived, and maternal mortality fell by more than 90 percent.
Then the quiet period ended. The deregulation of obstetric risk did not look like financial deregulation. It looked like birth autonomy. It looked like questioning medicalization. It looked, in some iterations, like ideological opposition to hospital birth itself. The result was an expansion of out-of-hospital birth settings with variable licensure, variable training standards, and almost no mandatory adverse event reporting.
I have published on this with my colleague Frank Chervenak. Using CDC natality data, we have shown repeatedly that planned home birth in the United States carries neonatal mortality rates several times higher than planned hospital birth. This is not a fringe finding. It is consistent across years, across datasets, across analytical approaches. What it has not produced, consistently, is policy change.
Opacity: The Information Nobody Has
Krugman identifies opacity as the core structural problem with private credit. Lenders do not have to disclose their books. Borrowers do not have to disclose their finances. “In effect, private loans are treated as interactions between consenting adults,” he writes. “The rest of us have no legal right, and, presumably, no need to know what took place.”
American obstetrics operates with similar opacity when it fails. There is no national mandatory system for reporting maternal deaths and near-misses equivalent to, say, the aviation industry’s safety reporting architecture. The NTSB investigates every commercial aviation fatality and publishes its findings publicly. No comparable body exists for obstetric deaths. Most states have maternal mortality review committees, but their findings are not uniformly reported, not uniformly public, and not uniformly acted upon.
I proposed a National Obstetric and Birth Safety Investigation framework, explicitly modeled on the NTSB, precisely because this gap exists. The response from professional societies has been, to put it gently, measured. The system has no strong interest in illuminating its own failures.
Institutional Amnesia and the Upton Sinclair Principle
Krugman invokes Upton Sinclair: it is difficult to get a man to understand something when his salary depends on his not understanding it. This is, as far as I can tell, the most clinically accurate sentence in his essay.
ACOG guidelines are written by committees of physicians whose institutions, careers, and malpractice exposure are shaped by those same guidelines. The result, which I have documented using the GAAP Score instrument in a series of posts comparing ACOG against RCOG and NICE guidance, is a framework that consistently scores lower on consent specification and accountability than its British counterparts. Not because American obstetricians are worse physicians. Because the guidelines serve a different primary function.
When an institution writes its own safety rules, enforces its own safety rules, and investigates its own failures, the quiet period does not last.
The Wrong Diagnosis Is Its Own Kind of Risk
Krugman’s analysis of financial risk includes a structural observation that maps almost exactly onto my long-standing argument about American maternal mortality. The conversation in obstetrics has focused heavily on racial disparities in maternal outcomes. Black women in the United States die in childbirth at rates roughly two to three times higher than white women. That disparity is real, it is documented, and it demands a response. But here is where the analogy to financial crisis becomes uncomfortably precise: we have been treating the symptom while protecting the system that produces it.
The dominant policy response has been a push for racial equity training, implicit bias workshops, and diversity initiatives inside hospitals and medical schools. These are not worthless. But they are also not the reform. They are the equivalent of teaching individual bankers to be nicer while leaving the shadow banking system intact.
The structural driver of the disparity is insurance, not interpersonal bias. Medicaid reimburses at roughly half the rate of private insurance. The best-resourced hospitals and the most experienced physicians have no financial incentive to concentrate their practices on Medicaid patients. Poor women, who are disproportionately Black and Hispanic, are therefore disproportionately cared for in under-resourced settings by providers with fewer tools, less support staff, and higher patient loads. This is not a secret. It is a known, tolerated feature of American healthcare finance.
The solution is not to ask individual physicians to examine their biases. The solution is equal access to the same quality of care for every pregnant woman in America, regardless of her insurance status, her zip code, or her income. Every other wealthy country has figured this out. Germany has figured it out. France has figured it out. The United Kingdom has figured it out. Their maternal mortality rates are a fraction of ours, and their racial disparities in obstetric outcomes are substantially smaller, not because their physicians attended more equity seminars, but because their systems do not ration access to safe care based on ability to pay.
When we point the entire reform conversation at racial equity and away from universal access to safe obstetric care, we are not solving the problem. We are making the cockroaches harder to find. We are giving the system a story that sounds serious, requires no structural change, and leaves the financial architecture that produces the disparity completely untouched.
Cockroaches Are Not a Metaphor
Krugman’s cockroach reference is not really about cockroaches. It is about the epistemology of systemic risk. When one lender fails, others are probably holding similar assets. When one mother dies from a preventable cause, others are probably at risk from the same preventable cause. The question is whether the system has the infrastructure to learn from the first failure before the cascade begins.
Financial systems learned this lesson the hard way in 2008. American obstetrics has not yet had its 2008. The maternal mortality numbers suggest it is overdue.
My Take
Krugman ends his essay by asking how many cockroaches there are. I will end mine by noting that in obstetrics, we have been reluctant to count. Mandatory national adverse event reporting. A true NTSB-equivalent for obstetric deaths. Insurance reimbursement reform that actually aligns financial incentives with equal access and outcomes. Guideline accountability that puts patient safety above institutional protection.
None of these are new ideas. All of them face the same resistance Krugman describes in finance: the people who would implement them are the people whose salary depends on not implementing them.
Krugman is worried about 2008. I am worried about the 700 or so women who will die in American delivery rooms this year from causes that, in most other wealthy countries, would not have killed them. The financial crisis had a recovery. Those women will not.