
“The Hospital Everyone Wants, and the Chaos That Comes With It” - ObI | The Digital Waiting Room


Reddit is where patients go at 2 a.m. when scared. I monitor dozens of communities for clinically meaningful posts: dangerous myths, gaps between belief and evidence, stories guidelines cannot capture. This series -- ObGyn Intelligence on Reddit -- dissects them against the literature, because ObGyns who ignore social media ignore the most unfiltered window into what patients think, fear, and do between appointments.
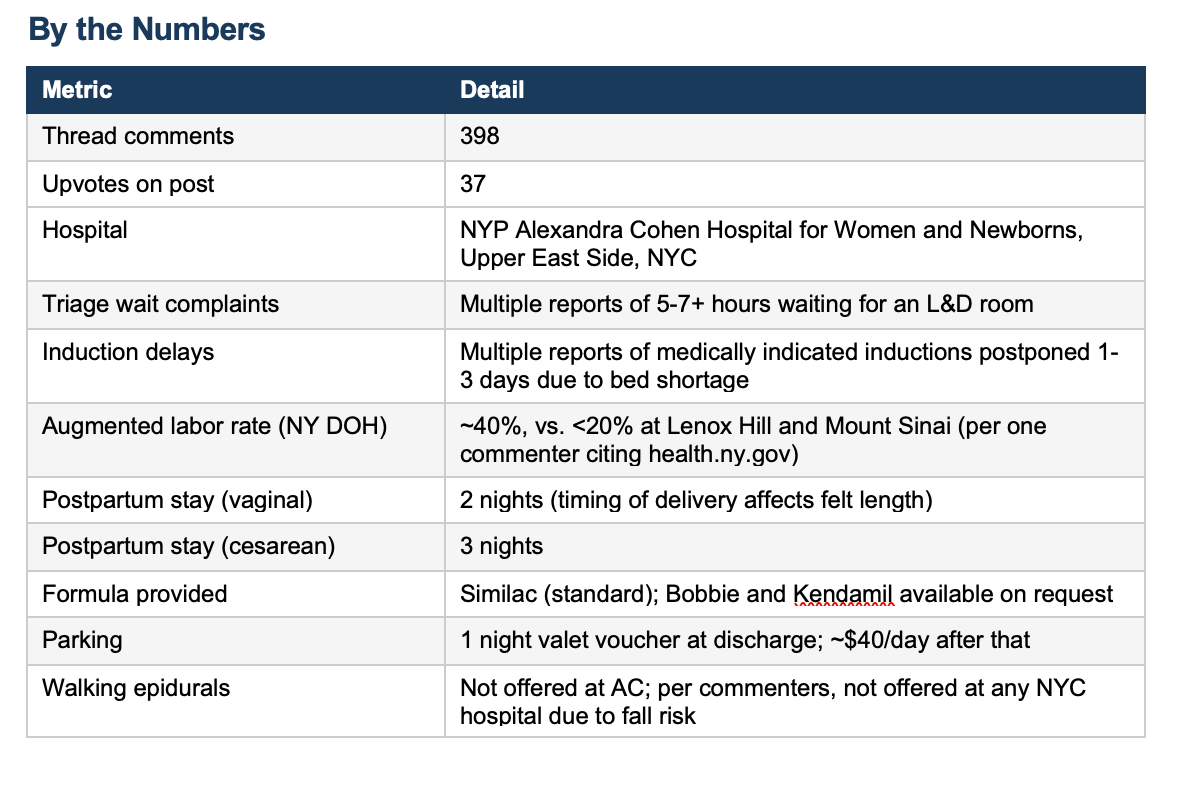
The r/nycparents subreddit has a dedicated megathread for NYP Weill Cornell’s Alexandra Cohen Hospital for Women and Newborns -- 398 comments and counting. A New York Magazine/The Cut article recentlty criticized the hospital for overcrowding, long triage waits, dismissive nurses, and one memorable case of in-room fleas. The Reddit community offers a messier and more nuanced picture: most people who delivered there loved it; most grievances are structural, not clinical.
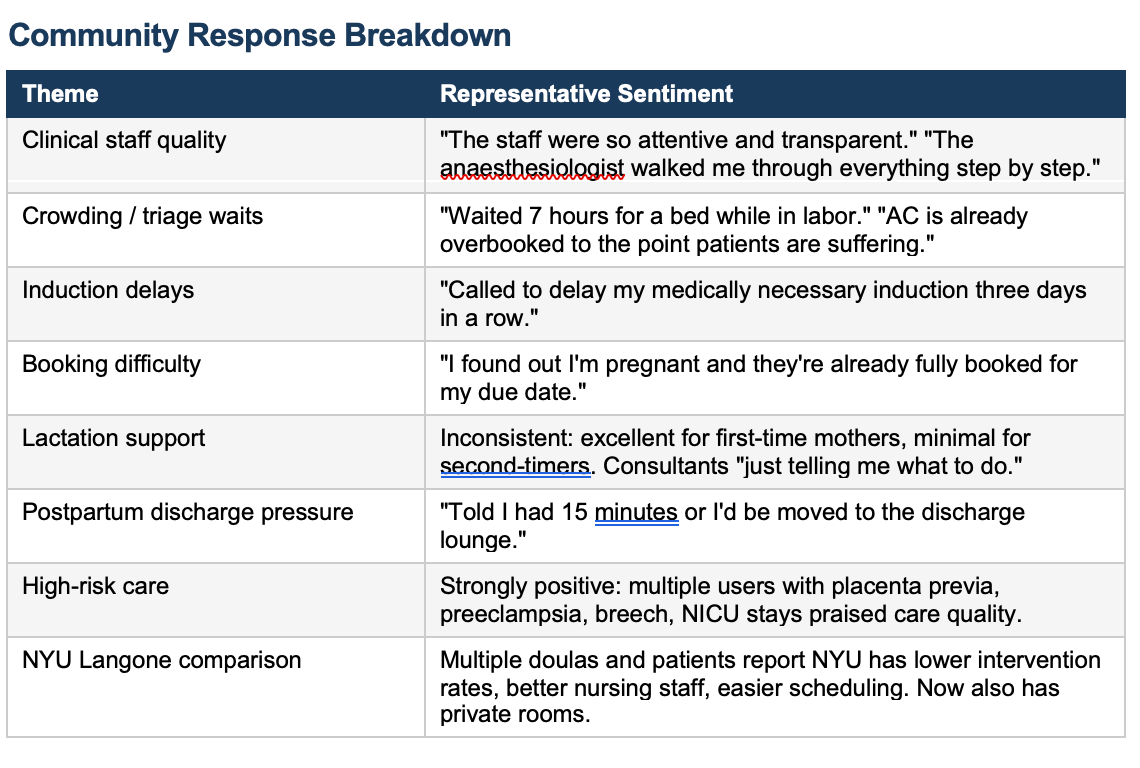
The staff gets high marks.
The system strains under its own popularity. Inductions get delayed or postponed entirely due to bed shortages. Postpartum stays feel rushed. Lactation support is inconsistent. And booking -- which requires calling individual physician offices rather than a central registry -- is a competitive sport that rewards those who pick up the phone at 17 days post-ovulation.
Commentary
The Alexandra Cohen thread is one of the more clinically useful things I’ve read on Reddit in a while. Not because the anecdotes are data -- they are not -- but because the patterns are too consistent to ignore, and some of them point directly at structural problems we know exist in high-volume obstetric units.
Start with the augmentation rate. One commenter cited New York State DOH data showing AC augments roughly 40% of labors -- double the rate at Lenox Hill and Mount Sinai. Augmentation means adding Pitocin or other agents after spontaneous labor has already begun. The stated rationale is usually failure to progress. The unstated pressure is bed turnover in an over-capacity unit. These are not always the same thing. The ARRIVE trial -- which AC’s high induction rates presumably reflect -- showed that elective induction at 39 weeks in low-risk nulliparous women did not increase cesarean rates in the trial population. But at the population level, looking at CDC natality data from 2016-2024, national cesarean rates went up as induction rates climbed. That is not a coincidence. It is what happens when a protocol designed for selected trial participants gets applied systemically to everyone.
The induction delay reports are arguably more alarming than the high rates. Multiple posters described medically indicated inductions -- not elective -- being postponed for one, two, even three days because there was no bed. One patient was called at midnight and told to be there in 30 minutes after three days of last-minute cancellations. This is not a scheduling inconvenience. A medically indicated induction exists because someone determined there was a clinical reason not to wait. Rescheduling it due to capacity is a form of rationing care, and it is happening without the patients necessarily understanding that is what is occurring.
The water outage mentioned by one commenter -- no running water, no flushing toilets, yet inductions and cesareans continued -- would be a major safety event at any hospital. It was flagged in the thread and then disappeared. That deserves more attention than it got.
On the positive side: the NICU care is uniformly praised. High-risk patients -- placenta previa, preeclampsia, breech presentation -- consistently describe excellent clinical management. This tracks with what we know about academic medical centers affiliated with major research institutions. They are organized to handle complexity. The problems emerge in the middle: low-risk patients who don’t need the tertiary resources but end up caught in the machinery built for those who do.
What It Means
Alexandra Cohen has become what happens when social media transforms a good hospital into a luxury brand. The Chanel bag joke circulating in the thread captures it: people want to deliver there for the private rooms and the prestige, but the unit was not built to absorb that volume, and the institutional response has been to keep accepting patients rather than to solve the throughput problem.
For patients, the practical implications are clear: book early -- as in, the week of your positive pregnancy test. Know which office your OB practices in, because at AC, you will likely be delivered by whoever is on call from your practice group, not your own doctor. Hire a doula, especially if you want to minimize interventions; multiple commenters noted that doulas were essential to navigating the culture. Advocate explicitly for your birth preferences because the default at a high-volume academic unit will trend toward intervention.
For the institution, the question is whether this is a problem they intend to fix. Posting a 40% augmentation rate and delaying medically indicated inductions due to bed shortage are not independent events. They are symptoms of the same capacity failure.
My Take
I have spent my career at institutions like this one -- academic centers where the clinical talent is real but the throughput pressure is also real. I know what it looks like when a unit is over-capacity and managing it through augmentation rather than expansion. I also know what it looks like when patients experience that management without understanding what is happening to them.
What strikes me most in this thread is the combination of individual clinical excellence and systemic dysfunction. The anesthesiologists are wonderful. The induction gets delayed for three days. Both things are true. They are not contradictory; they are exactly what happens when an institution’s operational model can no longer support its clinical ambitions.
The NYU comparison is instructive.
Doulas, who have no institutional loyalty and every incentive to recommend wherever their clients will have the best outcomes, are reportedly steering patients toward NYU. That is the kind of ground-level signal that should get administrators’ attention fast.