
The Rise of Performative Medicine
How screening for social determinants of health without the power to change them became one of obstetrics’ most practiced rituals


The Ritual
Somewhere in the United States right now, a pregnant woman is being handed a form. It asks whether she has enough food to eat. Whether she has stable housing. Whether she feels safe at home.
She answers the questions.
A medical assistant enters her responses into the electronic health record.
A clinician glances at the results, adds a note, and generates a referral to a social worker who may or may not have an opening this month.
The appointment ends.
The woman goes home to the same food insecurity, the same unstable housing, the same unsafe situation that she described on the form.
Nothing changed. But the chart is complete. The quality metric is satisfied. The box is checked.
This is performative medicine.
It looks like care.
It generates documentation that looks like care. It satisfies regulators who measure care by whether the question was asked, not by whether the answer produced any result. And it has become one of the defining rituals of modern obstetrics, applied most aggressively to the most vulnerable women in the system, the women whose problems are the largest, and whose access to solutions is the smallest.
Asking a woman whether she is hungry and then doing nothing about it is not compassionate medicine. It is data collection dressed up as a clinical encounter.
What Social Determinants of Health Actually Are
The term social determinants of health, abbreviated SDoH in the medical literature and on the quality metric dashboards of health systems across the country, refers to the non-medical conditions that shape health outcomes. Where a person lives. Whether she has reliable transportation. Her income and employment status. Her level of education. Whether her neighborhood is safe. Whether she has a social support network.
These factors are not peripheral to health.
They are central to it.
The evidence on this is clear and has been clear for decades. Poverty is a more powerful predictor of maternal mortality than almost any clinical variable we measure.
A woman’s zip code predicts her obstetric outcomes with more accuracy than her blood pressure or her BMI. Black women in the United States die in childbirth at approximately three times the rate of white women, a disparity that persists across income and education levels, that survives adjustment for clinical risk factors, and that reflects the accumulated weight of structural disadvantage that no prenatal vitamin and no screening tool will touch.
This is not a new insight. What is new is the medical profession’s response to it: the creation of a screening infrastructure that identifies social determinants of health systematically, documents them carefully, and then largely fails to address them in any meaningful way.
The Screening Industry
The push to screen for social determinants of health in clinical settings accelerated dramatically after the Affordable Care Act tied hospital reimbursement to quality metrics that included social risk factor documentation. Health systems across the country adopted validated screening tools: the PRAPARE protocol, the Accountable Health Communities Health-Related Social Needs Screening Tool, the Hunger Vital Sign. These are not bad instruments. They identify real problems with reasonable accuracy. The question has never been whether the screening tools work. The question is what happens after they do.
The United States Preventive Services Task Force has grappled openly with this tension. When it evaluated screening for food insecurity in clinical settings, it noted that the evidence for screening benefit was limited by the scarcity of interventions that could follow a positive result.
The same logic applies across the SDoH spectrum. Screening is easy. Solutions are hard. The medical profession has invested heavily in the former while largely deferring the latter to social service systems that are chronically underfunded, fragmented, and inaccessible to the patients most in need.
The USPSTF’s implicit framework for evaluating screening is whether a positive result leads to an effective intervention. For most social determinants of health, that intervention does not exist in most communities. The screening logic collapses.
Why Obstetrics Is Especially Vulnerable to This Failure
Obstetrics attracts more mandatory screening requirements than almost any other clinical specialty. The prenatal visit is a regulatory and quality metric magnet. Screens for depression. Screens for intimate partner violence. Screens for substance use. Screens for food insecurity. Screens for housing instability. Each added in response to a real problem, each backed by an argument that identification is the first step toward intervention.
The prenatal visit also runs under ten minutes of face-to-face time. A clinician moving through the required documentation has approximately 90 seconds to administer a screening tool, process the result, counsel the patient, place a referral if indicated, and document all of it before the next patient is already waiting. This is not a clinical encounter. It is a triage assembly line that has been retrofitted with a social work function it was never designed to perform.
The burden of this system falls hardest on the patients it is supposed to serve. High-risk women, women with Medicaid coverage, women at safety-net hospitals, women in rural areas with limited specialist access, these are the patients who screen positive most often and have the least access to the resources that would make a positive screen meaningful. They are asked the questions most frequently. They benefit from the answers least.
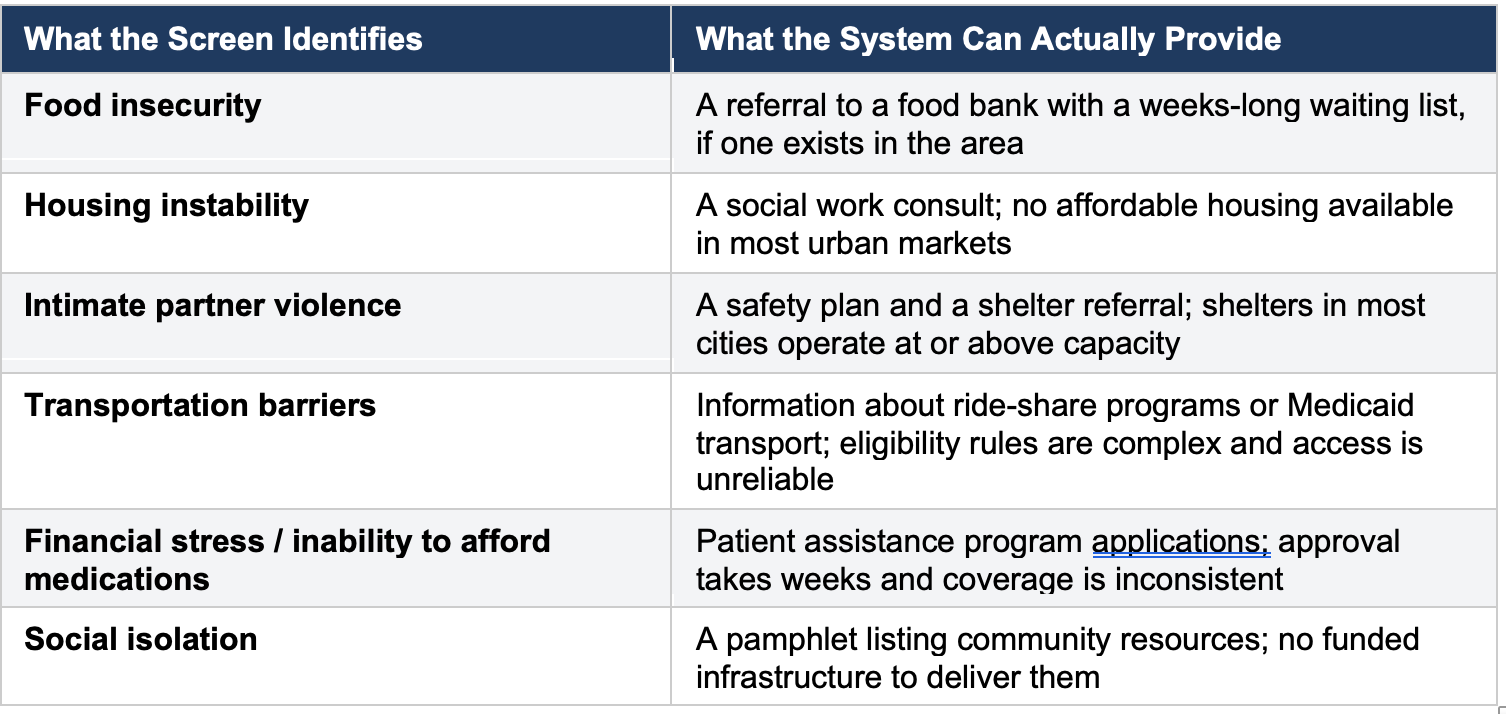
The table above is not a critique of the clinicians who complete these screens or the social workers who receive the referrals. It is a description of a structural mismatch that no amount of clinical effort will resolve. The problems identified by SDoH screening are not medical problems that have been overlooked. They are social and economic problems that have been handed to the medical system because no other system has been adequately funded to address them.
The Moral Hazard of Performative Medicine
There is a concept in economics called moral hazard: when a system creates the appearance of managing a risk, it can reduce the pressure to address that risk at its source. Performative medicine operates through a similar mechanism. When health systems can document that they screened for food insecurity, when quality dashboards show high rates of SDoH assessment, when accreditation bodies award credit for the process of screening, the urgency to address the underlying structural failures diminishes.
The clinician who asks a patient whether she has enough food and documents the answer has discharged her professional obligation as defined by the quality metric. She has not fed the patient. She has not changed the conditions that produced the food insecurity. She has, in a real sense, transferred the problem from the patient to the chart, where it will sit, documented and unresolved, until the next visit when it will be screened for again.
This is not a cynical observation about clinicians. Most of the physicians, midwives, and nurses who administer these screens do so with genuine concern for their patients. The cynicism is structural. A system that rewards documentation of a problem, rather than resolution of it, is a system that has organized itself around the performance of care rather than its substance.
When the metric is whether you asked the question, and not whether you changed the answer, you have built a machine for generating paperwork, not improving health.
The Institutional Benefit of the Status Quo
Health systems benefit from SDoH screening in ways that have nothing to do with patient outcomes. High rates of positive SDoH screens support claims of serving a high-risk population, which can influence reimbursement rates and justify additional resources. Documentation of social risk factors can serve as explanatory variables when outcomes are poor, providing institutional cover for mortality and complication rates that might otherwise invite scrutiny. Screening also generates data, and data has value in grant applications, research publications, and marketing materials about commitment to health equity.
None of this means SDoH screening serves no purpose. Identification can matter when interventions exist. But the current system has inverted the logical order: it screens first, systematically and at scale, and then treats the absence of solutions as a downstream problem for someone else to solve.
What Actually Moves Maternal Outcomes
The evidence on what improves obstetric outcomes is not ambiguous. It points consistently in a direction that has nothing to do with screening forms and everything to do with access, coverage, and quality of care.
Insurance That Actually Covers Care
Women with comprehensive insurance coverage have measurably better obstetric outcomes than women with limited coverage or no coverage. This is not a subtle effect. It operates across every outcome we measure: maternal mortality, severe maternal morbidity, preterm birth, low birth weight, postpartum complications. The gap between Medicaid coverage and private insurance in obstetric outcomes is real, persistent, and documented across multiple large datasets.
A woman who cannot afford her antihypertensive medication does not need a food insecurity screen. She needs a formulary that covers her medication without a copay she cannot pay.
Freedom to Choose a Skilled Clinician
The physician-patient relationship in obstetrics is not interchangeable. Outcomes vary across individual clinicians within the same institution. Continuity of care, seeing the same clinician across the prenatal period, is associated with better outcomes, higher patient satisfaction, and better identification of clinical risk.
A system that routes low-income women to whoever is available, across fragmented safety-net systems where continuity is nearly impossible to achieve, is a system that has decided that care quality is a function of what you can pay for. Screening those women for social determinants of health does not change that calculus.
Access to High-Quality Hospitals
Where a woman delivers matters enormously. High-volume centers with dedicated maternal-fetal medicine units, robust nursing ratios, and 24-hour anesthesia coverage have better maternal outcomes than low-volume community hospitals.
The geography of hospital quality in the United States maps almost perfectly onto the geography of income and race. Low-income women and Black women are more likely to deliver at hospitals with higher complication rates, not because of their clinical risk profiles, but because of where they live and what their insurance will cover. No screening tool changes which hospital a woman can access.
What Honest Medicine Looks Like
I am not arguing that clinicians should stop asking their patients about their lives. Context matters, as I have written before, and the clinician who understands a patient’s circumstances will always deliver better care than one who does not. The difference between contextual medicine and performative screening is the intent and the consequence.
Contextual medicine means asking about a patient’s life because the answer will change what you do in that visit. It means finding out that she stopped taking her medication because she cannot afford it, and changing the prescription. It means discovering that she does not have transportation, and calling in the prescription to a pharmacy near her home instead of one near the clinic. It means learning that she is not safe at home, and spending the rest of that visit, and the next one, making a safety plan that is specific to her situation.
Performative screening means asking the same questions because the quality metric requires it, documenting the answers because the electronic health record prompts the documentation, and generating a referral because the protocol specifies a referral, whether or not anyone in that patient’s community can act on it.
The distinction is not always visible from outside the encounter. Both produce documentation. Only one produces care.
Honest medicine requires us to say plainly what the evidence shows: if you want to improve maternal outcomes in the United States, the intervention is insurance, access, and quality of care. Not a questionnaire.
What Health Systems Should Stop Doing
Health systems should stop treating SDoH screening as a quality measure when the referral infrastructure does not exist to act on positive results. They should stop reporting high rates of SDoH screening to accreditation bodies as evidence of commitment to health equity when outcomes for the women who screen positive are unchanged. They should stop using SDoH documentation as an explanatory variable for poor outcomes without also accounting for what they did, or failed to do, with the information they collected.
What Health Systems Should Start Doing
Health systems that serve high-risk populations should invest in the infrastructure that makes a positive SDoH screen actionable: on-site or embedded social work with actual capacity, partnerships with food programs that can deliver, housing navigators with real relationships with local landlords and programs, legal services for patients with immigration concerns. These are expensive. They are also what the evidence says works. A screening program without this infrastructure is not a health equity initiative. It is a documentation program.
More fundamentally, the medical profession needs to be honest with policymakers, regulators, and the public about what medicine can and cannot do. Medicine can identify a woman who is food insecure. Medicine cannot feed her. Medicine can document that she lives in an unsafe neighborhood. Medicine cannot make it safe. Medicine can screen for intimate partner violence. Medicine cannot end it. The solutions to social determinants of health are social and political, not clinical. Pretending otherwise, by building screening programs that substitute for policy, is a disservice to the patients those programs claim to serve.
The Bottom Line
The United States spends more on maternity care per birth than any other high-income country and achieves outcomes that rank near the bottom of the same group. The maternal mortality rate is rising. Racial disparities in maternal outcomes are not closing. The response of the medical establishment to this failure has included, prominently, the expansion of social determinants of health screening in prenatal settings.
Screening is not the problem. The problem is a system that has adopted screening as a substitute for the structural changes that would actually matter: universal comprehensive coverage, payment models that support continuity and quality, equitable access to high-volume centers, and investment in the communities where the most vulnerable women live and give birth.
The woman who fills out a food insecurity screen at her prenatal visit deserves more than documentation of her hunger. She deserves a system that takes responsibility for what it finds. Until that system exists, the most honest thing we can say about SDoH screening in obstetrics is that we are very good at identifying problems we are not prepared to solve.
If the screen leads nowhere, the screen is not medicine. It is theater. And the audience paying the price is the patient.