
Twins Are Not One Pregnancy
Why chorionicity determines how carefully we must watch a twin gestation

Twin pregnancy means two fetuses share one uterus. Clinically, that sounds simple. Medically, it is one of the most complex situations in obstetrics. The key fact many patients never hear early enough is this: twin risk is not determined by the number of babies. It is determined by how the placenta is shared.
The first steps after twins are diagnosed is to determine the “chorionicity”.
Obstetricians therefore do not begin twin care by counting fetuses. We begin by identifying chorionicity, meaning how many placentas and how many amniotic sacs exist.
This is ideally determined by ultrasound at 11 to 14 weeks, because later the membranes become harder to interpret.
There are three biologic types of twins.
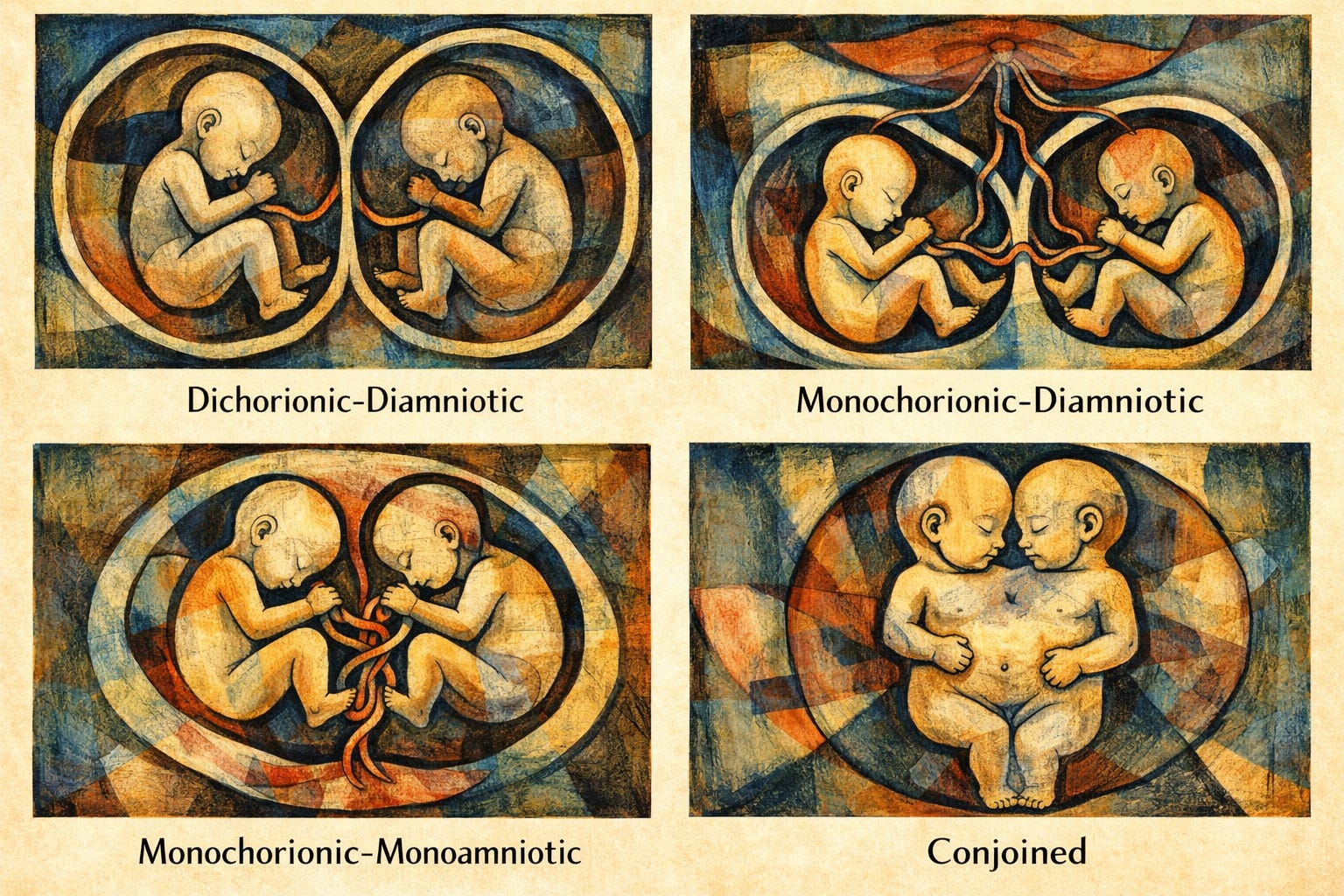
Dichorionic–diamniotic (di-di).
Each fetus has its own placenta and its own amniotic sac. This includes almost all fraternal twins and about one third of identical twins. The fetuses are physiologically separate. The risks are mainly those of uterine over-distention: preterm birth, maternal hypertension, and growth differences. These are the lowest-risk twins.
Monochorionic–diamniotic (mono-di).
The twins share one placenta but have separate sacs. This occurs when an embryo splits slightly later. Because the placenta is shared, blood vessels connect the twins. That single feature changes everything. One twin can transfuse blood to the other. This produces twin-to-twin transfusion syndrome, growth restriction of one twin, or sudden deterioration of both.
Monochorionic–monoamniotic (mono-mono).
The rarest form. One placenta and one sac. There is no separating membrane. The umbilical cords can entangle and compress. These pregnancies are uncommon but among the highest risk in modern obstetrics.
Coinjoined twins are part of MonoMono twins and are jopined anywhere on their bodies.
Monitoring follows directly from biology.
For di-di twins, surveillance resembles intensified singleton care.
• Anatomy scan at 18–22 weeks
• Growth ultrasound about every 4 weeks beginning at ~24 weeks
• Third-trimester antenatal testing around 32–34 weeks
• Delivery usually at 38 weeks if uncomplicated
For mono-di twins, the placenta requires active surveillance.
• Ultrasound every 2 weeks starting at 16 weeks
• At each visit: amniotic fluid in each sac and bladder filling
• Doppler assessment when concerns arise
The purpose is early detection of twin-to-twin transfusion syndrome and selective growth restriction. If TTTS develops, fetoscopic laser treatment may be needed. Delivery typically occurs around 36–37 weeks.
For mono-mono twins, monitoring becomes preventive rather than reactive.
• Ultrasound every 1–2 weeks in mid-pregnancy
• Intensive fetal surveillance in the third trimester
• Many centers hospitalize around 26–28 weeks for daily monitoring
The reason is cord entanglement, which cannot be predicted by growth scans. Planned cesarean delivery is usually recommended around 32–34 weeks before sudden cord compression occurs.
One important counseling point: twin monitoring is not about doing more ultrasounds for reassurance. It is about watching for specific pathophysiology unique to each placental type. A mono-di pregnancy can look normal one week and show early transfusion syndrome two weeks later. A mono-mono pregnancy can have normal growth and still face acute cord compromise. The schedule is designed around the biology of those risks.
Twin pregnancy therefore requires an early question at the first ultrasound:
not “Are both babies healthy?” but
“How many placentas are there?”
Once that is answered, the rest of prenatal care follows logically. The monitoring plan, visit frequency, and delivery timing are not arbitrary. They are a direct response to how the fetuses share circulation inside the uterus.