
Two Nations Divided by a Common Language. And Sometimes by a Health System.
The United States and the United Kingdom both practice modern medicine. Yet their cultures of care, responsibility, and decision making often feel like two professions separated by the same language.

Medicine in the United States and the United Kingdom appears similar on the surface. Both countries train highly skilled physicians, rely on scientific evidence, and care for patients within advanced hospital systems. Yet beneath that shared vocabulary lies a striking cultural divide.
Much like the linguistic differences between American and British English, the practice of medicine in the two countries reflects very different assumptions about authority, responsibility, and the role of the physician.
Even the language of medicine reveals the divide.
In the United States, a physician in training is called a resident, and a fully independent physician is an attending.
In the United Kingdom, since 2024, the term “resident doctor” is used for all doctors in postgraduate training, including both foundation doctors and specialty trainees, while the fully trained physician is called a consultant, equivalent to a US attending. Despite the shared term, a UK “resident doctor” spans a broader range of training stages than a US resident and is not a direct one-to-one equivalent.
An American patient goes to the emergency department, while in Britain the same patient goes to A&E. These differences may seem cosmetic, but they reflect different professional hierarchies and expectations about who ultimately carries responsibility for decisions.
The differences become even clearer on the hospital floor. In the United States obstetric care is typically delivered by a team that includes physicians, labor nurses, anesthesiologists, and neonatal specialists. Nurses play a central role during labor, continuously monitoring patients and assisting physicians.
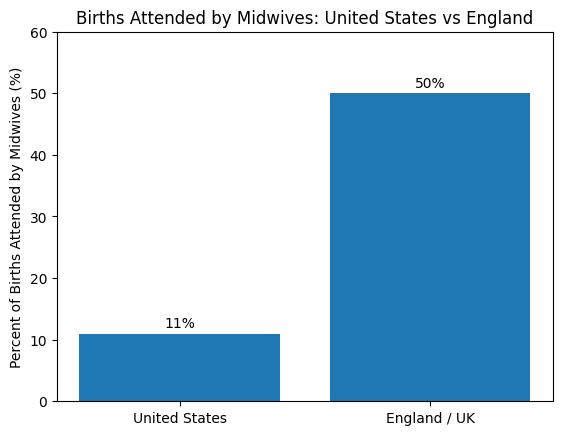
In many British maternity units the structure is different. Midwives are the primary professionals managing labor, often working independently, and physicians such as registrars or consultants are called when complications arise.
In general, physicians in British obstetric units do not have dedicated labor nurses assisting them in the same way American obstetricians do.
The contrast begins even earlier, during prenatal care. In Britain nearly all pregnant women receive care through the National Health Service. Prenatal visits, laboratory tests, ultrasound examinations, and delivery care are covered within a unified national system. Patients typically follow standardized care pathways coordinated by midwives and hospital-based obstetric services.
In the United States prenatal care depends heavily on insurance status. Some pregnant women receive care through private insurance plans, often with relatively broad access to specialists and imaging. Others rely on Medicaid, which finances a large share of births in the United States but varies widely by state in provider participation and coverage policies.
A smaller but important group of women begins pregnancy with no insurance at all, sometimes delaying prenatal care until Medicaid eligibility is established or until they present to hospital systems that provide safety-net services.
This difference shapes the experience of pregnancy. In Britain the question is rarely whether prenatal care will be covered. In the United States the question often becomes where that care will occur, which clinicians accept the insurance plan, and whether administrative barriers delay access to services.
The most obvious difference between the two systems remains structural. British medicine operates largely through the National Health Service. Physicians function inside a national system where access, resources, and clinical pathways are heavily standardized. American medicine developed in a more decentralized environment. Hospitals, insurers, and physician groups interact in a complex marketplace rather than within a single national framework.
This difference shapes clinical behavior. In the United Kingdom care is often organized around system stewardship. Guidelines and care pathways frequently determine what happens next.
In the United States physicians historically retained more individual authority in clinical decision making, even as administrative oversight and insurance constraints continue to grow.
The contrast is especially visible in obstetrics. American obstetrics traditionally emphasizes physician responsibility for individual outcomes. A clinician managing labor often carries personal legal and professional accountability for decisions made in that room. In the United Kingdom responsibility is more distributed across teams and systems of care, including a stronger institutional role for midwifery services.
Communication styles also diverge.
British medical culture tends to favor understatement, indirectness, and institutional language. American medicine often communicates more explicitly about risk, intervention, and individual decision making.
These differences can influence how clinicians frame uncertainty, how patients perceive autonomy, and how professional authority is exercised.
None of this means one system is inherently superior. Each reflects the history, law, and culture that produced it. British medicine grew inside a national health service designed after World War II to guarantee universal access. American medicine developed through a patchwork of private practice, academic centers, and insurance markets.
Yet the deeper question is philosophical. What does society expect a physician to be?
In Britain the physician often functions as a steward of public resources within a coordinated national service. In the United States the physician historically acted as an independent professional responsible primarily to the patient in front of them.
That difference still shapes attitudes toward guidelines, innovation, and clinical autonomy.
The irony is that both systems are changing. British physicians increasingly face workforce shortages and resource constraints within the NHS. American physicians increasingly practice within large health systems where administrative rules influence clinical choices.
In other words, the two traditions may slowly be converging.
Still, the cultural differences remain unmistakable. Spend time in a British hospital ward and then walk through an American labor unit. The language is the same. The textbooks are the same. The science is the same.
But the practice of medicine feels different.
Sometimes profoundly so.
LinkedIn tagline:
Two countries. Same science. Very different cultures of obstetric care.
Hashtags:
#Obstetrics #MedicalEthics #NHS #USHealthcare #HealthSystems #ClinicalResponsibility #ObstetricIntelligence
16:9 Image Prompt:
Split image of two maternity care settings. Left side shows a modern American labor and delivery unit with obstetricians and nurses reviewing fetal monitoring. Right side shows a British NHS maternity ward where midwives manage labor while a consultant obstetrician reviews a chart. Subtle visual cues of the US and UK flags in background lighting, clean professional hospital environment, editorial illustration style, soft natural light.
and add a couple sentences about division of care by insurances for hospitals too
Two Nations Divided by a Common Language. And Sometimes by a Health System.
Subtitle: The United States and the United Kingdom both practice modern medicine. Yet their cultures of care, responsibility, and decision making often feel like two professions separated by the same language.
Series: The Obstetric Intellect
Where ideas, evidence, and ethics meet to challenge assumptions in obstetrics.
Medicine in the United States and the United Kingdom appears similar on the surface. Both countries train highly skilled physicians, rely on scientific evidence, and care for patients within advanced hospital systems. Yet beneath that shared vocabulary lies a striking cultural divide. Much like the linguistic differences between American and British English, the practice of medicine in the two countries reflects very different assumptions about authority, responsibility, and the role of the physician.
Even the language of medicine reveals the divide. In the United States a young physician is a resident. In Britain the equivalent doctor is a registrar or senior house officer, and the senior physician is called a consultant, rather than an attending. An American patient goes to the emergency department, while in Britain the same patient goes to A&E. These differences may seem cosmetic, but they reflect different professional hierarchies and expectations about who ultimately carries responsibility for decisions.
The differences become even clearer on the hospital floor. In the United States obstetric care is typically delivered by a team that includes physicians, labor nurses, anesthesiologists, and neonatal specialists. Nurses play a central role during labor, continuously monitoring patients and assisting physicians. In many British maternity units the structure is different. Midwives are the primary professionals managing labor, often working independently, and physicians such as registrars or consultants are called when complications arise. In general, physicians in British obstetric units do not have dedicated labor nurses assisting them in the same way American obstetricians do.
The contrast begins even earlier, during prenatal care. In Britain nearly all pregnant women receive care through the National Health Service. Prenatal visits, laboratory tests, ultrasound examinations, and delivery care are covered within a unified national system. Patients typically follow standardized care pathways coordinated by midwives and hospital-based obstetric services.
In the United States prenatal care depends heavily on insurance status. Some pregnant women receive care through private insurance plans, often with relatively broad access to specialists and imaging. Others rely on Medicaid, which finances a large share of births in the United States but varies widely by state in provider participation and coverage policies. A smaller but important group of women begins pregnancy with no insurance at all, sometimes delaying prenatal care until Medicaid eligibility is established or until they present to hospital systems that provide safety-net services.
Insurance also shapes where women give birth. In the United States hospitals often have different patient mixes depending on the insurance coverage they accept. Some hospitals predominantly serve privately insured patients, while others function as safety-net institutions caring for large Medicaid or uninsured populations. As a result, the distribution of obstetric patients across hospitals can mirror the structure of the insurance system itself.
In Britain such financial sorting rarely occurs. Because the NHS finances maternity care nationally, pregnant women are generally directed to hospitals based primarily on geography and service capacity rather than insurance status.
The most obvious difference between the two systems remains structural. British medicine operates largely through the National Health Service. Physicians function inside a national system where access, resources, and clinical pathways are heavily standardized. American medicine developed in a more decentralized environment. Hospitals, insurers, and physician groups interact in a complex marketplace rather than within a single national framework.
This difference shapes clinical behavior. In the United Kingdom care is often organized around system stewardship. Guidelines and care pathways frequently determine what happens next. In the United States physicians historically retained more individual authority in clinical decision making, even as administrative oversight and insurance constraints continue to grow.
The contrast is especially visible in obstetrics. American obstetrics traditionally emphasizes physician responsibility for individual outcomes. A clinician managing labor often carries personal legal and professional accountability for decisions made in that room. In the United Kingdom responsibility is more distributed across teams and systems of care, including a stronger institutional role for midwifery services.
Communication styles also diverge. British medical culture tends to favor understatement, indirectness, and institutional language. American medicine often communicates more explicitly about risk, intervention, and individual decision making. These differences can influence how clinicians frame uncertainty, how patients perceive autonomy, and how professional authority is exercised.
None of this means one system is inherently superior. Each reflects the history, law, and culture that produced it. British medicine grew inside a national health service designed after World War II to guarantee universal access. American medicine developed through a patchwork of private practice, academic centers, and insurance markets.
Yet the deeper question is philosophical. What does society expect a physician to be?
In Britain the physician often functions as a steward of public resources within a coordinated national service. In the United States the physician historically acted as an independent professional responsible primarily to the patient in front of them.
That difference still shapes attitudes toward guidelines, innovation, and clinical autonomy.
The irony is that both systems are changing. British physicians increasingly face workforce shortages and resource constraints within the NHS. American physicians increasingly practice within large health systems where administrative rules influence clinical choices.
In other words, the two traditions may slowly be converging.
Still, the cultural differences remain unmistakable. Spend time in a British hospital ward and then walk through an American labor unit. The language is the same. The textbooks are the same. The science is the same.
But the practice of medicine feels different.
Sometimes profoundly so.