
“What’s Something You Were Surprised Pregnanancy Impoved" ObI: The Digital Waiting Room

Reddit is where patients go at 2 a.m. when scared. I monitor dozens of communities for clinically meaningful posts: dangerous myths, gaps between belief and evidence, stories guidelines cannot capture. This series -- ObGyn Intelligence on Reddit -- dissects them against the literature, because ObGyns who ignore social media ignore the most unfiltered window into what patients think, fear, and do between appointments.
Summary
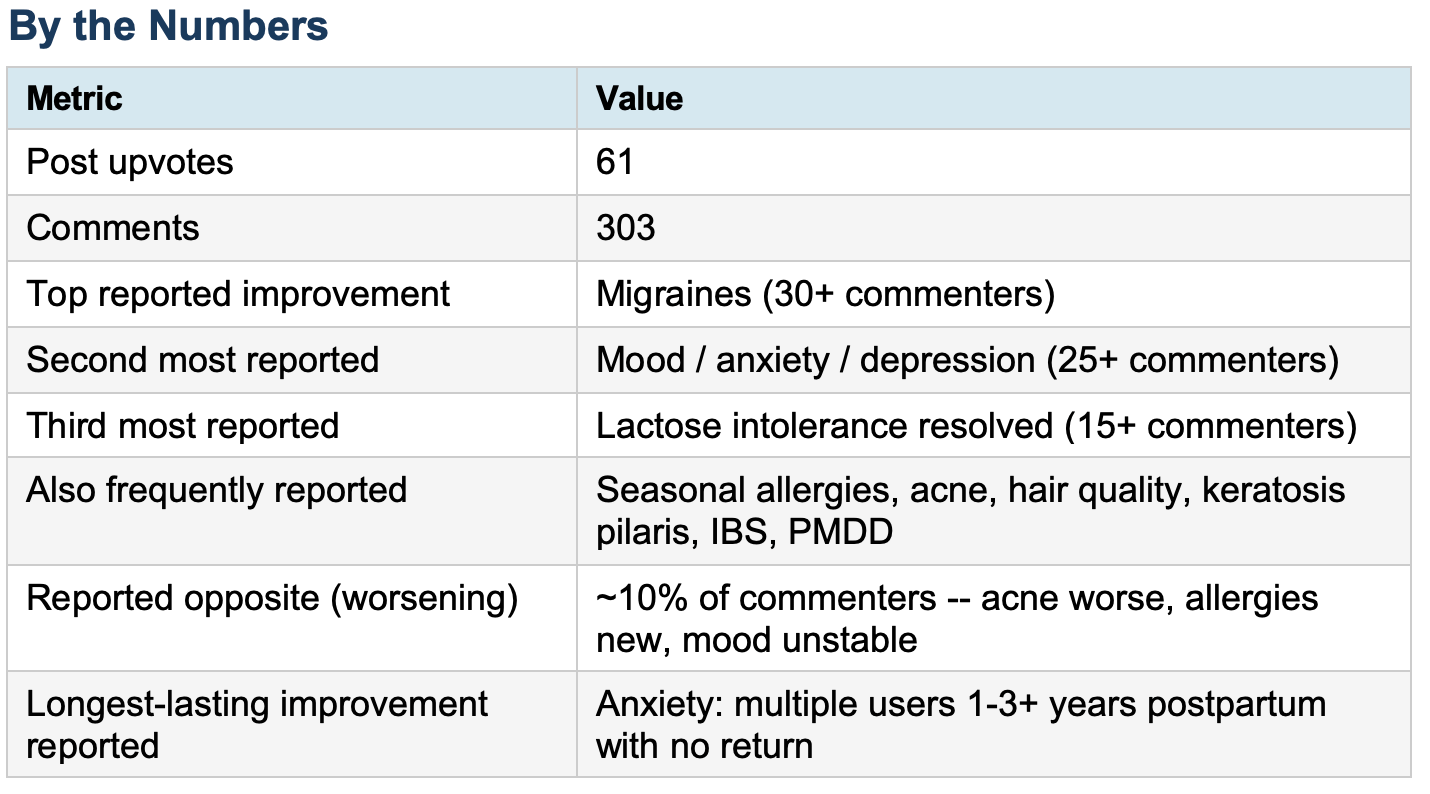
A user at 9 weeks pregnant noticed on Reddit something unexpected: her spring allergies -- severe enough to require daily antihistamines from March through June -- had essentially vanished. The post landed on r/pregnant and drew 303 comments in under 24 hours. What poured in was not advice. It was testimony. Hundreds of women describing conditions that had improved, disappeared, or transformed during pregnancy: migraines gone, depression lifted, lactose intolerance reversed, anxiety quieted, autoimmune skin conditions cleared. A few dozen noted the opposite -- everything got worse. But the dominant signal was striking: pregnancy, for many women, functions as an uninstructed biological experiment, reshaping the immune system, the nervous system, and the hormonal environment in ways that clinical medicine has not fully mapped. These women are noticing. Their doctors, for the most part, are not asking.
Evidence-Based Commentary
What this thread documents is not surprising to reproductive physiologists. It is, however, largely invisible in obstetric practice -- and that gap is worth examining.
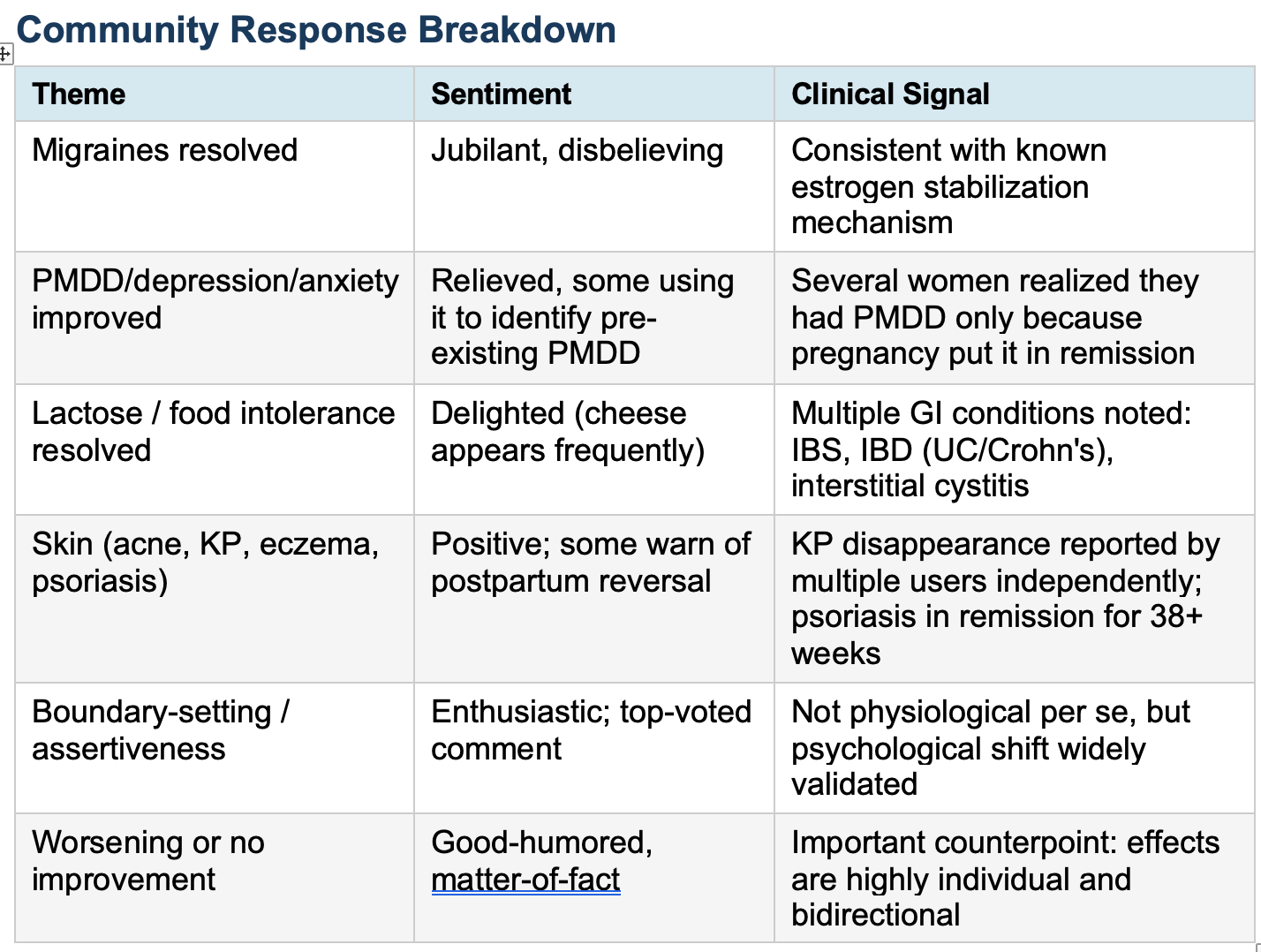
Migraines. This was the most frequently cited improvement, mentioned by more than 30 commenters independently. The mechanism is well established. Migraines in women of reproductive age are predominantly hormonally triggered, driven by estrogen fluctuations across the menstrual cycle. Pregnancy produces stable, progressively rising estrogen levels with no cyclical drops -- exactly the environment migraine-prone brains prefer. Multiple controlled studies have confirmed that migraine frequency decreases significantly in the second and third trimesters in the majority of affected women. The first trimester can be worse due to early hormonal flux, and several commenters noted this accurately. Postpartum return is common and often rapid. Women on migraine preventatives who discontinue them for pregnancy should have a specific plan for postpartum management before delivery -- this conversation is not happening often enough.
Mood disorders, anxiety, and PMDD. The second major theme is more complex and clinically important. Dozens of women described marked improvement in depression, generalized anxiety, and what several identified as PMDD. Multiple commenters noted -- correctly -- that pregnancy puts PMDD in remission because there is no luteal phase. Premenstrual dysphoric disorder is fundamentally a disorder of cyclical hormone sensitivity; remove the cycle, the disorder goes quiet. Several women in this thread reported discovering they had PMDD precisely because pregnancy revealed the contrast. This is a legitimate diagnostic insight, and it should be explicitly discussed: women with mood symptoms that track their cycle who get pregnant and feel dramatically better should be informed of the likely return of those symptoms postpartum, and should have a postpartum mental health plan in place before discharge. The evidence for postpartum mood disorder risk in women with pre-existing PMDD or anxiety is substantial. One commenter observed that progesterone is described as “nature’s Xanax” -- this is a popular simplification of a real phenomenon. Progesterone metabolizes to allopregnanolone, a positive allosteric modulator of GABA-A receptors. The sharp postpartum drop in allopregnanolone is now understood to be a central mechanism in postpartum depression, which led directly to the development of brexanolone (Zulresso), the first FDA-approved treatment specifically for PPD. Women who feel unusually well during pregnancy are not imagining it. They should be told why, and warned what to expect.
Do this postpartum screening and mental health plan.
Immune-mediated conditions: allergies, KP, psoriasis, eczema, IBD. Pregnancy is a state of profound immune reorganization. The fetus is, immunologically speaking, a semi-foreign graft. To prevent rejection, the maternal immune system shifts toward tolerance -- reducing Th1 (cell-mediated, pro-inflammatory) activity and upregulating Th2 (humoral, anti-inflammatory) responses. This shift is well documented. The clinical consequences reported in this thread follow predictably. Autoimmune and inflammatory conditions that are Th1-driven -- psoriasis, rheumatoid arthritis, some eczema variants, Crohn’s disease -- tend to improve during pregnancy. Conditions that are Th2-driven -- atopic dermatitis in some forms, asthma -- may worsen. Multiple commenters reported keratosis pilaris (KP) disappearing during pregnancy; the proposed mechanism involves hormonal effects on keratinocyte differentiation, though the evidence base is limited. The interstitial cystitis improvement noted by one commenter is consistent with case reports and small series in the literature. Ulcerative colitis remission during pregnancy, noted by another user, is well documented -- the pregnancy-associated Th2 shift suppresses the inflammatory cascade driving UC. Women with IBD should be counseled pre-pregnancy that their disease behavior may change and should continue specialist monitoring throughout.
Lactose intolerance. This was reported by 15 or more commenters and is probably the most mechanistically interesting finding in the thread. Lactase -- the enzyme required to digest lactose -- is produced in the small intestinal brush border. There is evidence that estrogen and progesterone influence intestinal lactase expression and GI motility. Pregnancy also significantly slows GI transit time, which may allow more time for incomplete lactase activity to process lactose before symptoms develop. The clinical implication is modest but worth knowing: some women who believe they cannot tolerate dairy may tolerate it better during pregnancy. Blanket dairy restriction in pregnant women who experience lactose intolerance prenatally is not necessarily warranted -- they may be able to tolerate dietary calcium sources they had previously avoided.
What nobody is telling these women. Across 303 comments, the pattern is unmistakable: women are experiencing significant changes in established medical conditions during pregnancy, they are surprised by these changes, and they are sharing them with each other because no one told them to expect them. Prenatal care systematically addresses what pregnancy will add -- nausea, heartburn, back pain, fatigue, edema. It rarely addresses what pregnancy may temporarily resolve and what will return. The postpartum period is when the reckoning arrives: migraines come back, PMDD returns, psoriasis flares, anxiety resurfaces. Women who were not prepared for this are blindsided. The informed consent failure is not dramatic -- no one is harmed acutely -- but it is real. Preparing patients for postpartum biological rebound is part of comprehensive obstetric care, and most practices are not doing it.
What It Means
Pregnancy temporarily reorganizes the immune system, stabilizes estrogen, floods the brain with neurosteroids, and alters GI function. For millions of women, this means conditions they have managed for years -- sometimes their entire adult lives -- go quiet for nine months. The clinical community knows the mechanisms. It is not translating that knowledge into patient counseling. Women are learning from each other that migraines, PMDD, IBS, psoriasis, and anxiety may improve during pregnancy, and they are being surprised when these conditions return postpartum. Obstetric providers should be having explicit conversations about anticipated postpartum rebound for any patient whose pre-existing condition improved during pregnancy. That conversation belongs in the third trimester, not in the postpartum ER.
My Take
I have spent 50 years in obstetrics. I have watched women become different people during pregnancy -- calmer, clearer-headed, migraine-free, pain-free, allergy-free -- and I have watched them come back six weeks postpartum asking what happened to them. We knew what was going to happen. We did not tell them.
The top comment in this thread -- 288 upvotes -- was from a woman who said pregnancy taught her to say no. The second was about migraines. The third was about leg hair. This is what patients think about. This is what they notice. They are running an n-of-1 experiment on themselves every pregnancy, collecting data that medicine should be systematically gathering.
What strikes me most is the PMDD thread.
Multiple women realized they had PMDD only because pregnancy made it disappear.
That is a diagnostic finding. It belongs in a chart.
It should trigger a postpartum screening and mental health plan.
How many women who are “just hormonal” before pregnancy actually have PMDD, go undiagnosed because no one frames the question correctly, and then crash postpartum without any preparation? The answer is: more than we are catching. Reddit figured this out in the comments. We should be doing it in the office.