
Who Gets the Final Say? Clashing Over Management for Fetal Distress
What is the right ethical thing to do when a doctor refuses to follow good medicine

It was late in the evening when my pager went off. A labor and delivery nurse was on the other end, her voice urgent but steady. “Doctor, I think the fetus is in trouble. Too much pitocin. The patient’s doctor won’t stop the infusion.”
I headed straight to the unit.
A Rare but Tense Scenario
Pitocin—synthetic oxytocin—is one of the most common medications used in labor. It stimulates contractions, often making the difference between a stalled labor and a successful vaginal delivery. But like any powerful medication, it carries risks. Too much can cause hyperstimulation of the uterus, reducing blood flow to the fetus and leading to heart rate changes that signal distress.
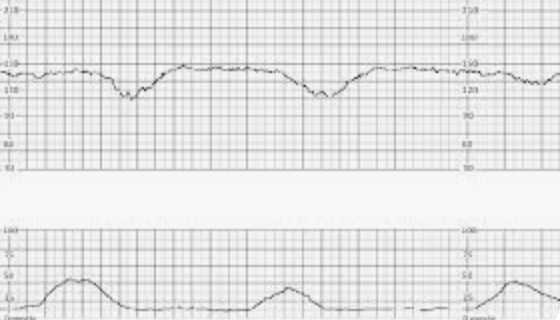
In this case, the nurse was right: the fetal heart tracing showed late decelerations, a warning sign that the baby was not tolerating the contractions well. The protocol was clear: stop or reduce the pitocin.
But the patient’s doctor refused.
The Huddle
As director of the labor and delivery unit, I convened a team huddle. Nurses, residents, anesthesiologists—everyone was present. We reviewed the strip together. The consensus was unanimous: the pitocin needed to be stopped.
Still, the physician of record insisted on continuing the infusion, dismissing concerns. This was more than a medical disagreement. It was a collision of professional responsibility, patient safety, and hierarchy.
Taking Over
At moments like these, hesitation can cost lives. My role was not just administrative but ethical: I had to weigh respect for a colleague’s autonomy against the obligation to protect the patient and her baby.
Ultimately, I intervened, taking over management of the case. The pitocin was discontinued, supportive measures were provided, and labor progressed more safely. Hours later, the patient delivered a healthy baby. Relief filled the room, but the ethical unease lingered.
Why This Matters
Such conflicts are extremely rare, but when they happen, they reveal fault lines in the practice of obstetrics:
Hospital Protocol vs. Physician Judgment
Protocols exist for a reason: they reflect evidence-based consensus. Yet some physicians see them as suggestions rather than rules, especially if they believe their clinical experience justifies a different course.Patient Autonomy
Informed consent means the patient has the right to understand and participate in decisions. But when medical professionals disagree in front of her, autonomy is undermined. The patient may not know whom to trust.The Chain of Command
Nurses are trained to advocate for patients, and most hospitals now have “chain of command” protocols that allow them to escalate concerns when they believe a doctor’s orders endanger safety. But exercising that right can be intimidating, especially in the face of authority.
Where Team Training Fits In
Events like this also highlight the importance of team training and simulation in obstetrics. It is not enough to know the medical protocols. Teams must practice what happens when people disagree, when hierarchy collides with urgency, and when communication breaks down.
Simulation Scenarios
Many hospitals now use high-fidelity simulation to rehearse obstetric emergencies—postpartum hemorrhage, shoulder dystocia, or fetal distress. These drills allow teams to practice both technical maneuvers and communication strategies under stress.Speaking Up and Escalation
Nurses must feel empowered to voice concerns. Residents must be able to challenge attendings respectfully. Attendings must learn how to disagree without escalating into paralysis. These are not instincts—they are skills that require practice.Breaking the Hierarchy
Traditional medicine is hierarchical: the doctor gives orders, others follow. But obstetric emergencies move too quickly for rigid hierarchy. In a well-trained team, leadership is situational—shifting fluidly to whoever recognizes the problem first.The “Time-Out” for Fetal Distress
Just as surgical teams use a “time-out” before an operation, labor and delivery teams can use structured pauses during emergencies. A quick huddle to review the tracing, voice concerns, and confirm next steps can prevent conflict from derailing care.
Lessons for Practice
Empower Nurses
When a nurse believes something is unsafe, the system must guarantee a pathway for action without fear of retaliation. Their voices often provide the first line of defense.Foster a Culture of Safety
Team huddles and shared review of fetal tracings are not just procedural—they build a collective ethic of accountability.Clarify Leadership in Emergencies
A labor floor is not the place for prolonged debates. Every hospital should define who has the authority to step in when immediate action is required.Train Together, Not Apart
Too often, doctors, nurses, and anesthesiologists train in silos. Real safety comes when everyone rehearses the same scenarios, hears the same language, and learns to anticipate each other’s moves.Prioritize the Baby
Ultimately, the fetus has no voice. It is our professional responsibility to advocate on its behalf, even when that means uncomfortable conflict.
Reflection
That night ended well, but the unease remained. Taking over from another physician is one of the hardest decisions in obstetrics. It risks professional conflict, even legal consequences. Yet sometimes doing nothing carries the far greater risk of harm.
Team training is what allows us to manage these rare but high-stakes scenarios without chaos. It teaches us that safety does not depend on any one person but on a culture where every voice matters and the patient—both mother and baby—remain at the center.
So here is the question I leave with you: when a baby’s life is on the line, who gets the final say—the physician of record, the hospital, or the team at the bedside?