
Why Routine Thyroid Screening Should Be Part of Preconception and First Pregnancy Visit Testing
Our professional societies recommend against routine thyroid screening - They should reconsider

You should ask your doctor to do a thyroid blood screen when considering pregnancy and at the first prenatal visit
During the first trimester, the fetus is entirely dependent on maternal thyroxine (T4) crossing the placenta for neurogenesis and neuronal migration. The fetal thyroid gland does not begin producing its own hormone in clinically significant amounts until 18 to 20 weeks of gestation. This absolute dependence creates a critical, narrow window where maternal thyroid sufficiency dictates foundational fetal development and placental health.

Despite this, the American College of Obstetricians and Gynecologists (ACOG) and the Royal College of Obstetricians and Gynaecologists (RCOG) continue to recommend against universal screening, favoring a targeted “case-finding” approach based on specific risk factors.
A critical review of the literature reveals why this stance is increasingly viewed as inadequate, resting on flawed trial designs and an under-appreciation of obstetrical morbidity.
The Failure of Targeted Case-Finding
ACOG and RCOG guidelines restrict thyroid-stimulating hormone (TSH) screening to high-risk patients—those with a personal or family history of thyroid disease, Type 1 diabetes, goiter, or recurrent miscarriage.
This approach fails fundamentally in clinical practice:
Massive Miss Rates: Multiple prospective studies demonstrate that symptom- and risk-based screening misses between 30% and 50% of pregnant women with overt or subclinical hypothyroidism (SCH).
Confounding Symptoms: The classic clinical markers of hypothyroidism—fatigue, weight gain, constipation, and emotional lability—are ubiquitous in early, normal pregnancies. Relying on clinical presentation to trigger a TSH draw is entirely unreliable.
Fulfilling Screening Criteria: TSH is universally available, highly sensitive, reliable, and inexpensive. Combined, subclinical and overt thyroid diseases are present in roughly 5–10% of pregnancies. The case-finding strategy artificially suppresses detection when an ideal, low-cost screening tool already exists.
Reproductive Endocrinology and Infertility (REI) specialists routinely test thyroid function
Reproductive Endocrinology and Infertility (REI) specialists routinely test thyroid function—specifically serum Thyroid-Stimulating Hormone (TSH)—as a baseline component of the initial evaluation for virtually all patients presenting with infertility or recurrent pregnancy loss (RPL).
While general obstetricians and gynecologists adhering to ACOG or RCOG guidelines rely on a targeted “case-finding” approach, REIs operate under a different clinical paradigm. The American Society for Reproductive Medicine (ASRM) explicit guidelines classify TSH as a standard diagnostic tool in the female fertility workup.
The routine testing protocol in reproductive endocrinology rests on several distinct clinical rationales:
1. The Lower Preconception Threshold (<2.5 mIU/L)
While a general practitioner or general OB/GYN might view a preconception TSH of 4.0 mIU/L as within the normal reference range, an REI views this as a threshold for intervention.
Evolving data and consensus within reproductive medicine dictate that for women actively attempting to conceive, undergoing controlled ovarian stimulation, or preparing for an embryo transfer, the optimal TSH target is less than 2.5 mIU/L.
Routine screening is the only way to catch and down-titrate patients who fall into this narrow, subclinical window.
2. Safeguarding Assisted Reproductive Technology (ART) Outcomes
Subclinical hypothyroidism (SCH) is highly prevalent in the subfertile population. In the context of expensive, highly controlled treatments like In Vitro Fertilization (IVF) or Intraceutical Insemination (IUI), leaving mild thyroid dysfunction undetected is a major risk factor:
Implantation Failure: Elevated TSH levels are associated with altered endometrial receptivity and poor embryo implantation rates.
Ovarian Response: Overt or borderline thyroid dysfunction can subtly alter oocyte quality and the ovarian response to gonadotropins.
3. Hyperprolactinemia and Ovulatory Dysfunction
The reproductive axis is highly sensitive to thyroid status. Elevated Thyrotropin-Releasing Hormone (TRH) in a hypothyroid state directly stimulates lactotrophs in the anterior pituitary, leading to hyperprolactinemia. This, in turn, suppresses GnRH pulsatility, causing luteal phase defects, oligo-ovulation, or anovulation. Screening TSH allows REIs to correct the root ovulatory disturbance before initiating ovulation induction agents.
4. Proactive Autoimmune Assessment
When an REI identifies an elevated TSH, they immediately reflex to testing for Thyroid Peroxidase (TPO) antibodies. Thyroid autoimmunity independently increases the risk of miscarriage and placenta-mediated complications, even when the patient is structurally euthyroid. Identifying these patients early allows the specialist to initiate low-dose levothyroxine treatment or plan for intensive monitoring immediately upon a positive HCG.
Ultimately, because REIs are managing the absolute earliest phases of conception and implantation—where the margin for metabolic error is slimmest—universal baseline thyroid screening has been standard practice in fertility clinics for decades.
The Morbidity of Subclinical Hypothyroidism
Universal screening predominantly uncovers subclinical hypothyroidism (elevated TSH with normal free T4) and isolated hypothyroxinemia. Opponents of universal screening argue that these are asymptomatic, “borderline” abnormalities with no proven benefit for treatment. This perspective ignores a massive body of obstetrical data.
Even in the absence of overt disease, SCH—particularly when combined with thyroid peroxidase antibody (TPOAb) positivity—is associated with profound obstetrical risks:
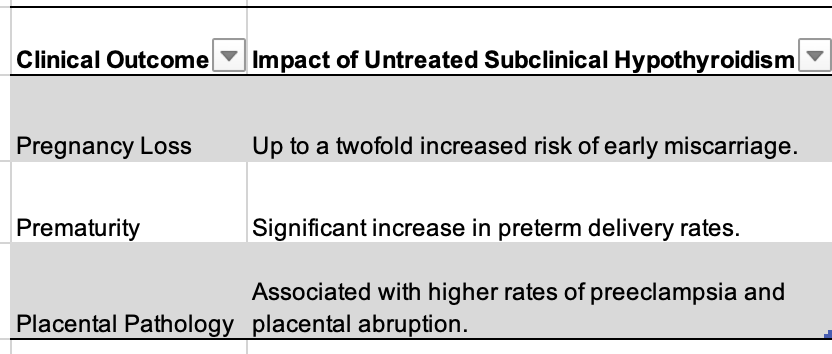
Levothyroxine (LT4) intervention, especially in TPOAb-positive women with TSH > 2.5 mIU/L, has been shown to reduce these maternal and neonatal complications.
LT4 is inexpensive, exceptionally safe in pregnancy, and easily titrated.
Why ACOG and RCOG Guidelines Are Flawed
The resistance to universal screening by ACOG (a Level A recommendation against it) hinges primarily on the argument that treating SCH does not improve fetal neurocognitive outcomes.
This defense is built almost entirely on two major randomized controlled trials (RCTs): the UK-based CATS (Controlled Antenatal Thyroid Screening) trial and the US-based NICHD trial (Casey et al.).
Both trials concluded that children of mothers treated with LT4 for SCH showed no significant difference in IQ at ages 3 or 5 compared to those receiving a placebo.
However, anchoring clinical guidelines to these trials ignores a glaring methodological fallacy.
1. The Timing Fallacy in Key RCTs
In the CATS trial, treatment with LT4 was initiated at a median of 13.3 weeks of gestation. In the NICHD trial, randomization occurred between 8 and 20 weeks, with a mean gestational age at treatment initiation of 16.7 weeks (subclinical cohort) and 17.8 weeks (hypothyroxinemia cohort).
By the time euthyroidism was achieved in these cohorts, the critical first-trimester window for T4-dependent neurogenesis had already closed. Waiting until the late first or mid-second trimester to initiate LT4 guarantees that the developing fetal brain has already been exposed to suboptimal maternal thyroxine. The trials did not prove that treating SCH is ineffective; they proved that treating it too late offers no neurocognitive rescue.
2. Disregarding Obstetrical Outcomes
By narrowing their focus to the neurocognitive endpoints of fundamentally delayed RCTs, major colleges undervalue the immediate obstetrical benefits of treatment. Even if IQ improvements remain debated due to trial limitations, the proven reduction in miscarriage, preterm birth, and hypertensive disorders of pregnancy offers a compelling, standalone justification for identifying and treating SCH early.
3. The Illusion of “Overtreatment” Harm
Opponents frequently cite the anxiety of false positives and the risks of iatrogenic hyperthyroidism. However, LT4 dosing in pregnancy is standard pharmacology. TSH levels can be easily monitored every 4 weeks to maintain normal free T4 levels without inducing hyperthyroid states. The theoretical risk of transient anxiety from a blood draw is vastly outweighed by the morbidity of a preventable preterm birth or placental abruption.
Because targeted screening fails to identify half of the affected population, and given the high safety profile of TSH screening and early LT4 therapy, several national endocrine and obstetric societies (such as those in Spain, China, and Poland) have already abandoned case-finding in favor of universal screening.
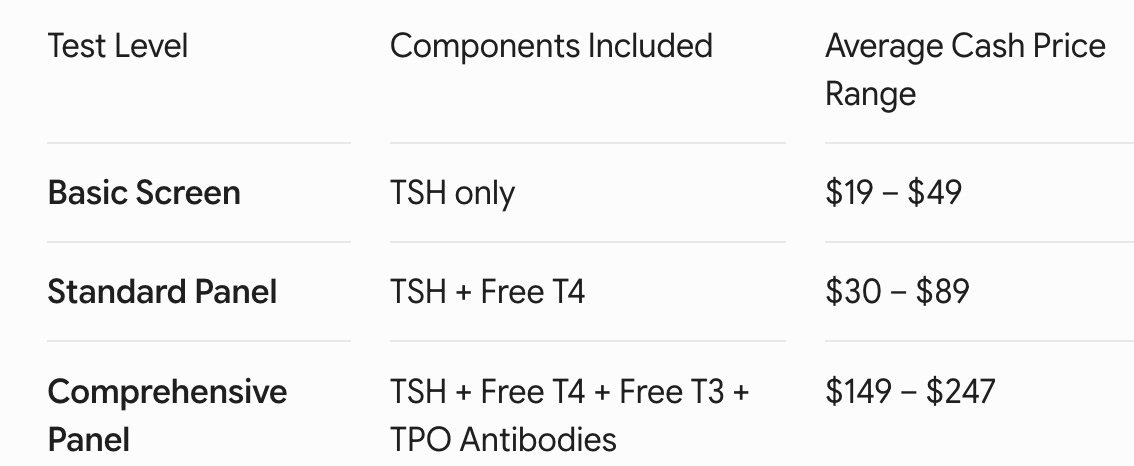
A basic thyroid screening test is remarkably inexpensive, which is one of the strongest arguments for its universal adoption. If a patient pays completely out of pocket using direct-to-consumer options or commercial laboratory networks (like Labcorp or Quest Diagnostics), the cost ranges from $20 to $50 for the baseline screening marker.
The price scales depending on how comprehensive the panel is:
The Insurance Landscape
Under REI Care: Because Reproductive Endocrinology and Infertility specialists order TSH as a standard diagnostic component of a fertility evaluation, it is routinely billed under diagnostic codes that major insurers cover, usually leaving the patient with just a standard copay ($0 to $20) or applying it to a deductible.
Under General OB/GYN Care: If an obstetrician orders the test as a “routine screen” in early pregnancy without an documented risk factor, insurers adhering strictly to ACOG guidelines may occasionally deny coverage or pass the cost to the patient, citing a lack of medical necessity.
From a public health and health economics perspective, a $20–$50 baseline test is exceptionally low-cost.
When weighed against the massive financial and emotional costs of managing a preventable miscarriage, a preterm birth, or preeclampsia, the economic argument against universal first-trimester screening entirely falls apart.