
You Were Told You Have PCOS. Now What?
A practical guide to getting a real diagnosis, protecting your future fertility, and knowing which doctor to see first.

Christina is 31 years old. Her periods have been irregular since college. Her doctor told her she probably has polycystic ovary syndrome, handed her a pamphlet, and said to come back when she is ready to try to get pregnant.
She left with a diagnosis and no plan.
That is a clinical failure, and it happens every day.
PCOS affects between 8% and 13% of women of reproductive age, making it the most common hormonal disorder in women. It is also one of the most mismanaged. The diagnosis is often handed out too loosely or, conversely, missed entirely. The next steps are rarely explained. And the window between diagnosis and the decision to conceive, which can span years, is almost never used well.
If you have been told you have PCOS and you want to have children someday, this post is for you.
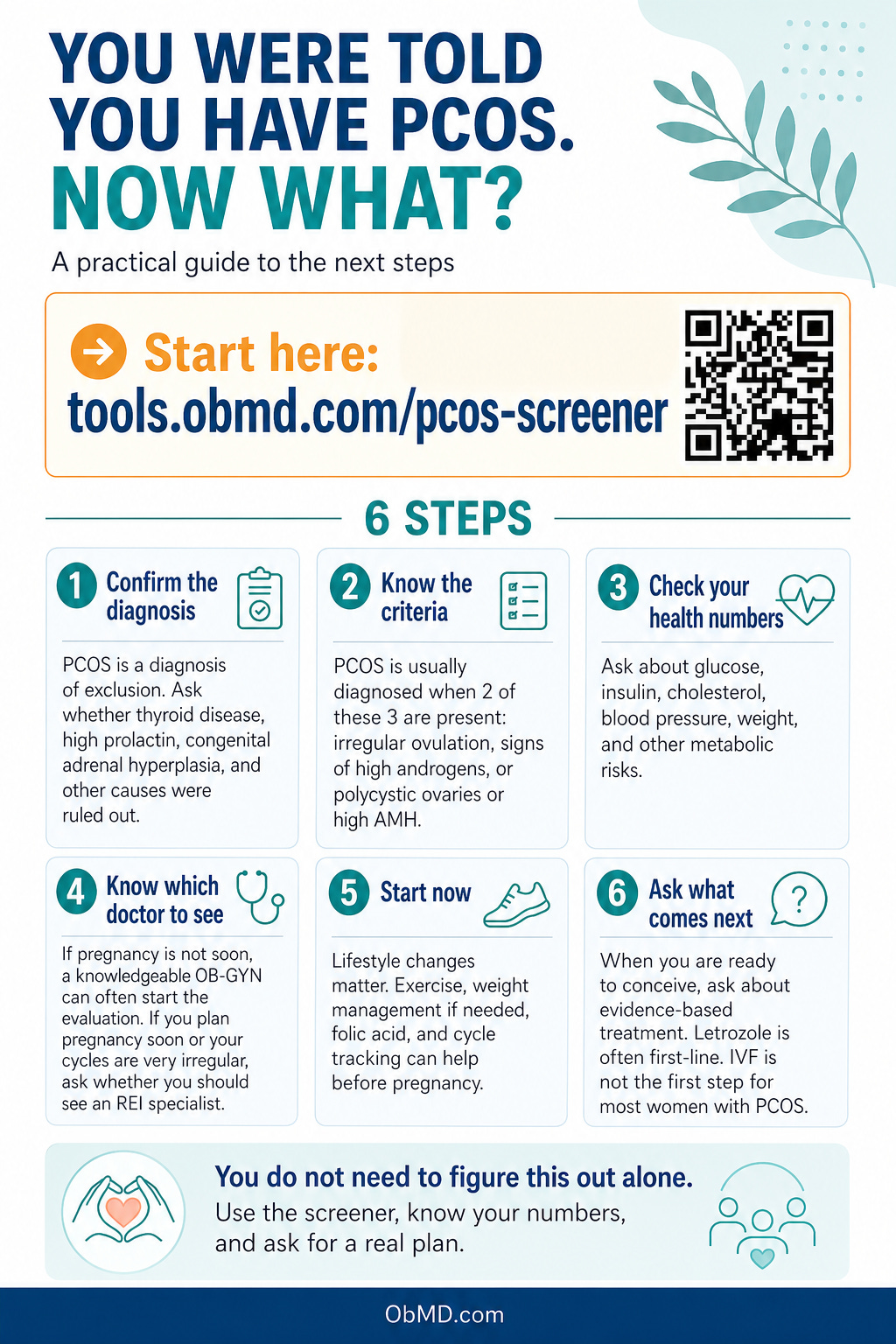
Step One: Make Sure the Diagnosis Is Real
This matters more than most patients are told. PCOS is a diagnosis of exclusion. That means before anyone can properly say you have it, other conditions that look similar must be ruled out: thyroid disease, elevated prolactin, congenital adrenal hyperplasia, and androgen-secreting tumors, among others. Some of these carry serious implications of their own and need different treatment entirely.
The standard criteria for PCOS diagnosis are the Rotterdam criteria, updated and strengthened by international evidence-based guidelines in 2023.
You can use the PCOS Screener at tools.obmd.com/pcos-screener to work through the Rotterdam criteria yourself before your appointment.”
Under these criteria, you need at least two of the following three findings, with other causes excluded:
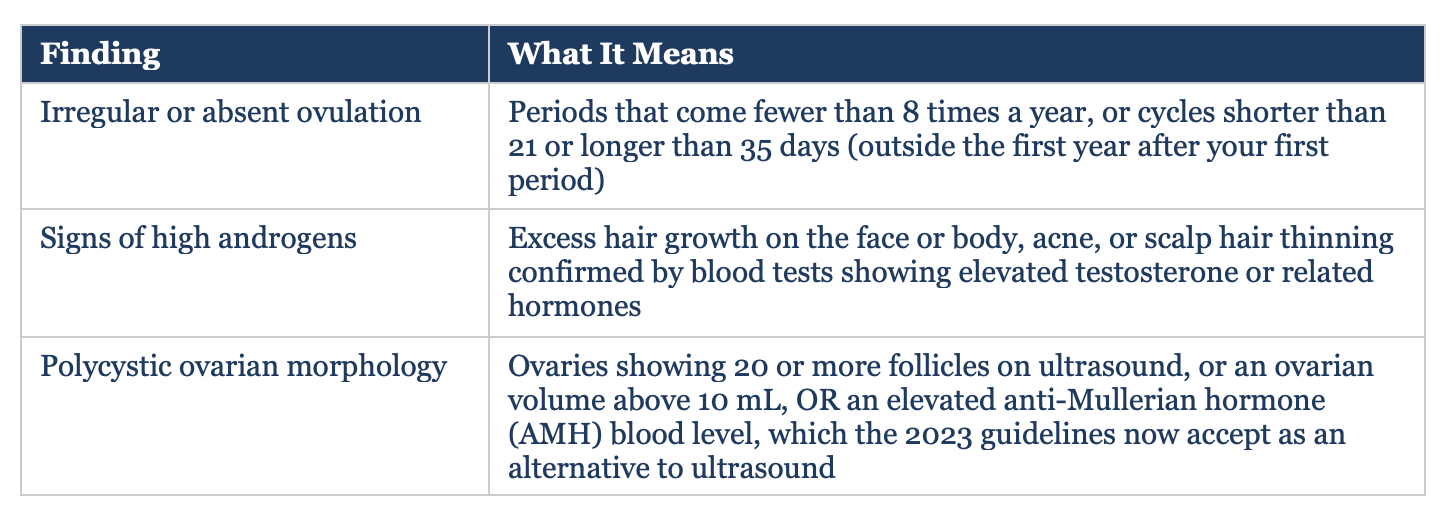
A critical point: having polycystic-looking ovaries on ultrasound alone does not mean you have PCOS. Up to 20% of women with completely normal cycles have ovaries that look polycystic on ultrasound. The word polycystic on your radiology report is not a diagnosis.
If your doctor made the diagnosis based only on an ultrasound or on irregular periods without checking your hormones and ruling out other causes, the diagnosis deserves a second look.
Which Doctor Should You See?
This depends on where you are in your journey.
If you are not trying to conceive in the next six months, a knowledgeable general obstetrician-gynecologist can absolutely manage your PCOS evaluation and initial treatment.
The priorities at this stage are confirming the diagnosis correctly, checking your metabolic health (fasting glucose, insulin, lipids, blood pressure), addressing symptoms like excess hair growth or acne, and starting lifestyle changes that will improve your hormonal environment before you ever need fertility treatment.
If you are planning to conceive within the next six months to a year, or if your cycles are so irregular that you have difficulty tracking ovulation at all, a referral to a reproductive endocrinologist and infertility specialist (REI) is reasonable.
An REI has the training and tools to assess your ovarian reserve, monitor ovulation induction cycles, and manage the full spectrum of PCOS-related fertility challenges.
You do not need to go directly to an REI. You do not need IVF as a first step. But you should not wait until you have been trying to conceive for a year before getting a proper evaluation, which is the standard advice given to women under 35. Women with known ovulatory dysfunction, which is what PCOS produces, should seek evaluation after six months of trying without success, or sooner if cycles are very irregular.
What You Can Do Right Now, Before You Are Ready to Try
The gap between PCOS diagnosis and fertility treatment is not dead time. It is the most powerful window you have. Here is what the evidence supports:
Weight and Metabolic Health
If your BMI is above 25 kg/m, losing 5% to 10% of your body weight through diet and exercise has been shown to restore ovulatory cycles, reduce testosterone levels, and improve insulin sensitivity. A structured 20-week exercise program in one systematic review improved ovulation rates by 49%. These are not small effects. Lifestyle change is not a consolation prize while you wait for medication. For overweight women with PCOS, it is the most powerful first intervention available.
If your weight is already in a healthy range, structured aerobic and resistance exercise still improves insulin sensitivity and androgen levels. The mechanism matters regardless of weight: PCOS is fundamentally tied to insulin resistance, which disrupts the hormonal signals that control ovulation.
Folic Acid and Preconception Nutrients
Start 400-800 micrograms of folic acid daily now. If you have a family history of neural tube defects or are taking certain medications, your doctor may recommend 4 milligrams daily instead. This is straightforward, inexpensive, and evidence-based. Do not wait until you get a positive pregnancy test to start.
Track Your Cycles
Irregular cycles in PCOS mean that ovulation is unpredictable, not that it never happens. Tracking with basal body temperature, ovulation predictor kits, or a period tracking app gives you and your doctor real data. If you are ovulating occasionally, that information changes your management. If you are not ovulating at all, that information also changes your management.
Metformin
Metformin is an insulin-sensitizing medication that has been used in PCOS for decades. The 2023 international guidelines support its use to improve menstrual regularity, reduce androgen levels, and lower the risk of gestational diabetes during a future pregnancy. It is not a fertility drug by itself, but it improves the hormonal environment and can help restore more regular cycles in women with insulin resistance. Ask your doctor whether metformin makes sense for you now, before you need fertility treatment.
When You Are Ready to Try: What Fertility Treatment Looks Like for PCOS
PCOS is the leading cause of anovulatory infertility.
Anovulatory means you are not releasing eggs regularly.
The good news: anovulatory infertility responds well to treatment. Most women with PCOS who want to conceive do so, often without IVF.
The treatment ladder for PCOS-related infertility, as established by the 2023 international guidelines, looks like this:
1. Lifestyle modification first, in women with a BMI above 25 kg/m
2. Letrozole (an aromatase inhibitor) as first-line oral ovulation induction
3. Clomiphene with or without metformin as second-line oral therapy
4. Gonadotropins (injectable hormones) or ovarian drilling surgery as second-line procedures
5. IVF as third-line therapy, when other approaches have failed or there is another indication for IVF
The NEJM landmark trial by Legro and colleagues (2014) established letrozole as superior to clomiphene for ovulation induction in PCOS. In that randomized controlled trial of 750 women, letrozole produced a cumulative live birth rate of 28% compared to 19% with clomiphene over five treatment cycles. Letrozole also carried a lower rate of twin pregnancies (3% versus 7%). If your doctor is still recommending clomiphene as the first choice, that recommendation is behind the evidence by a decade.
IVF is not a first step. It is expensive, physically demanding, and carries risks. The 2023 international guidelines are explicit: IVF should be offered only when other ovulation induction therapies have failed or when there is a separate reason IVF is needed. Women with PCOS who do go to IVF should receive single embryo transfer given the underlying pregnancy risks PCOS carries, including gestational diabetes, preeclampsia, and preterm birth.
One More Thing Most Doctors Do Not Mention
A fertility evaluation is never just about you. Before any treatment starts, your partner’s semen analysis should be done. About one in three cases of infertility involves a male factor. Starting ovulation induction without checking sperm first is putting the cart before the horse. Insist on this evaluation early.
My Take
A PCOS diagnosis handed over without a management plan is a missed opportunity. The years between diagnosis and a decision to conceive are not empty time. They are your best chance to improve your hormonal environment, protect your metabolic health, and position yourself for the simplest fertility path possible.
You do not need an REI on day one.
You need a clinician who will confirm the diagnosis properly, rule out other causes, check your metabolic numbers, and have an honest conversation about what your cycles are actually doing.
If that conversation does not happen, find someone who will have it.
When you are ready to conceive, letrozole is where the evidence points. Lifestyle change before that is not optional noise. It is the intervention with the best safety profile and no cost. And IVF, despite what fertility clinic marketing sometimes implies, is not the default destination for PCOS. For most women, it is not the destination at all.
Know your diagnosis. Know your numbers. And do not accept a pamphlet as a plan.
References
1. Teede HJ, Tay CT, Laven JJE, et al. Recommendations from the 2023 International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2023;108(10):2447-2469. doi: 10.1210/clinem/dgad463
2. Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus Clomiphene for Infertility in the Polycystic Ovary Syndrome. N Engl J Med. 2014;371(2):119-129. doi: 10.1056/NEJMoa1313517
3. Jalilian A, Kiani F, Sayehmiri F, Sayehmiri K, Khodaee Z, Akbari M. Prevalence of polycystic ovary syndrome and its associated complications in Iranian women: A meta-analysis. Iran J Reprod Med. 2015;13(10):591-604. [VERIFY for exact global prevalence figure]
4. Balen AH, Morley LC, Misso M, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update. 2016;22(6):687-708. doi: 10.1093/humupd/dmw025
5. Lim SS, Hutchison SK, Van Ryswyk E, Norman RJ, Teede HJ, Moran LJ. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2019;3(3):CD007506. doi: 10.1002/14651858.CD007506.pub4
6. Deng Z, Hu X, Li P, You Y, Zhong X, Guo C. Impact of lifestyle interventions on reproductive and psychological outcomes in women with polycystic ovary syndrome. Medicine (Baltimore). 2025. doi: 10.1097/MD.0000000000041247
7. Teede H, Deeks A, Moran L. Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010;8:41. doi: 10.1186/1741-7015-8-41